

Posture Correction Therapy and Pelvic Floor Muscle Function Assessed by sEMG with Intravaginal Electrode and Manometry in Female with Urinary Incontinence
- PMID: 36612691
- PMCID: PMC9819097
- DOI: 10.3390/ijerph20010369
Posture Correction Therapy and Pelvic Floor Muscle Function Assessed by sEMG with Intravaginal Electrode and Manometry in Female with Urinary Incontinence
Abstract
Introduction: The aim of the study was to assess the influence of the implemented therapeutic programme, which consisted of body posture correction and of change of habits, on the pelvic floor muscle function in women with stress urinary incontinence.
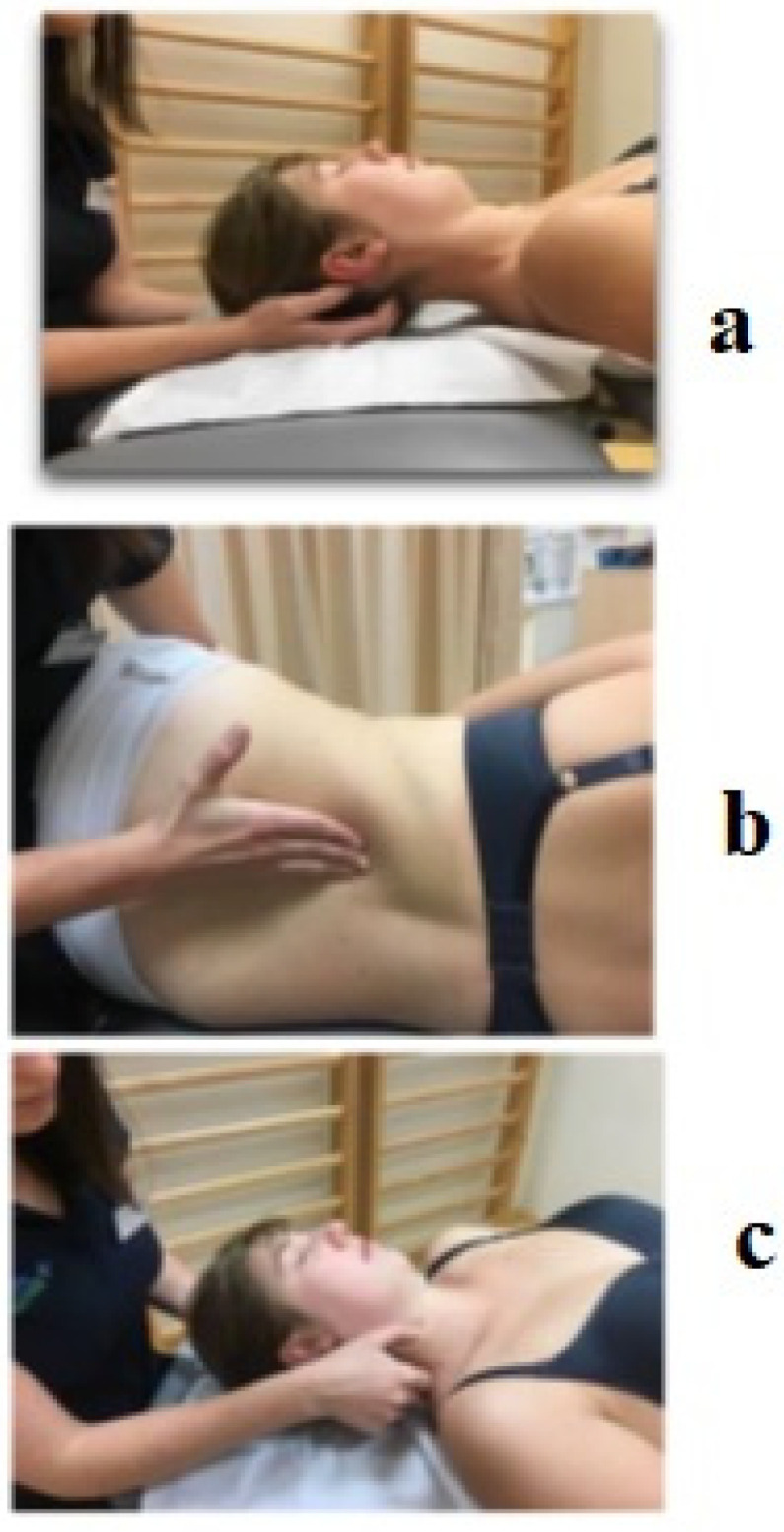
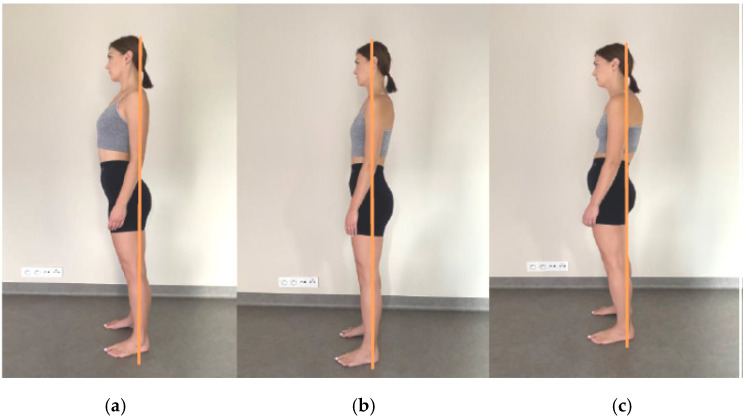
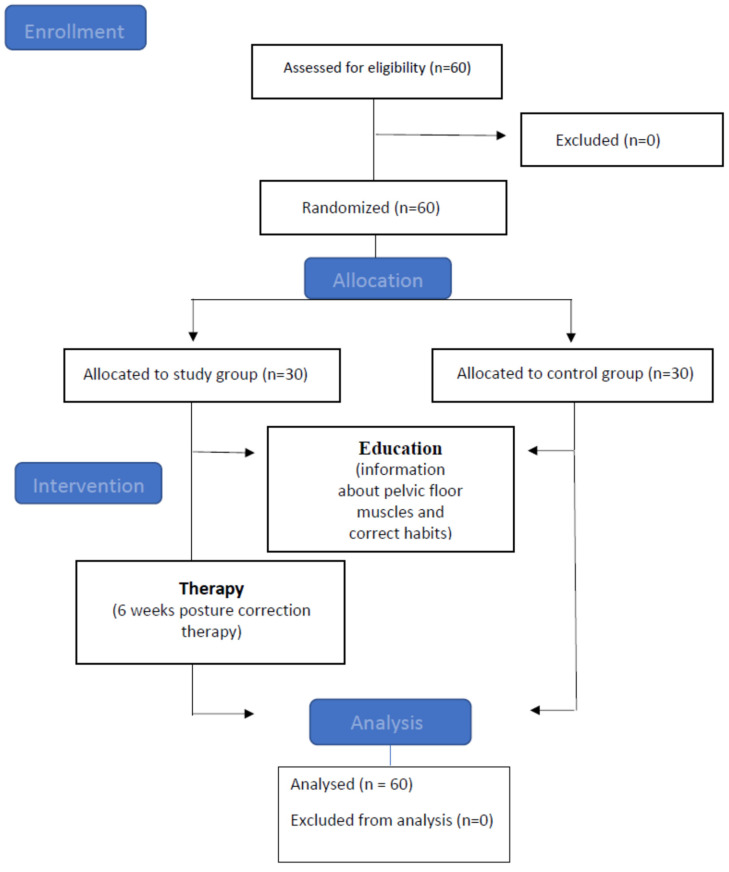
Material and methods: The 60 women were randomly divided into two groups: the study population and the clinical control group (subjects received envelopes with numbers of the group: 1- study population aged 38.3 ± 5.54, 2- clinical control group aged 35.5 ± 4.7. We used the following research methods: A personal questionnaire with subjects' demographics and with questions related to the type of work, physical activity, childbirths and any issues related to the pelvic floor (pre-test), Pelvic floor muscle assessment with the use of the PERFECT Scheme and the Oxford scale palpation examination, sEMG with intravaginal electrode and manometry with an intravaginal probe-pre-test and post-test. Subjective assessment of body posture in the sagittal plane according to the McKenzie methodology.
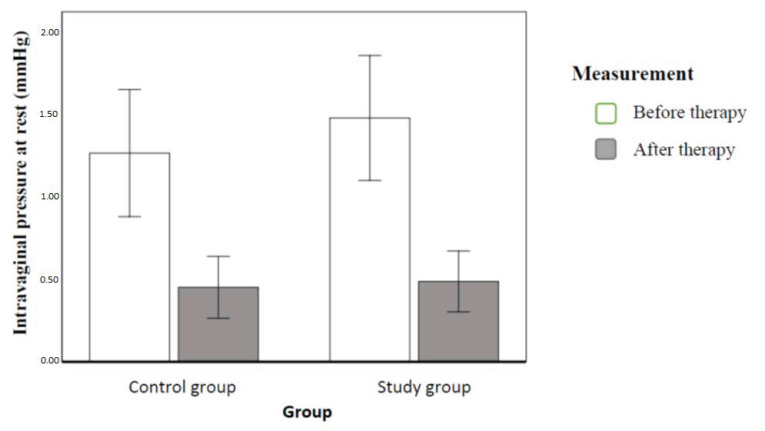
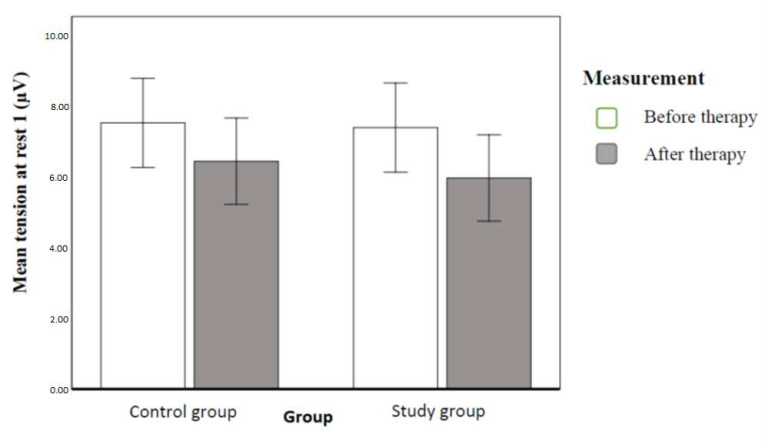
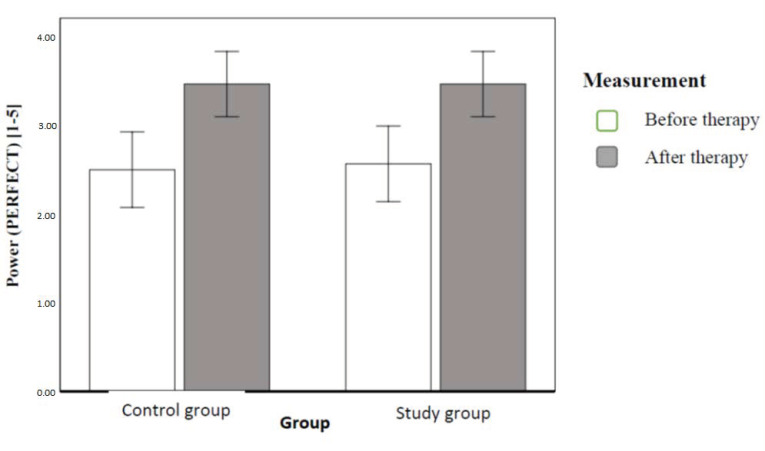
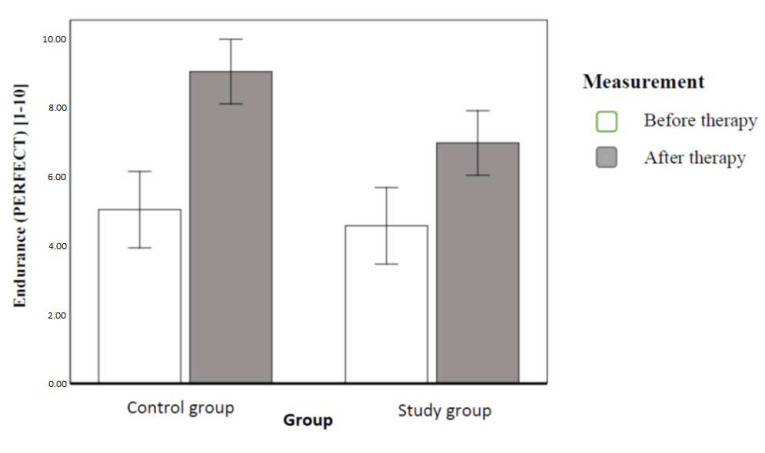
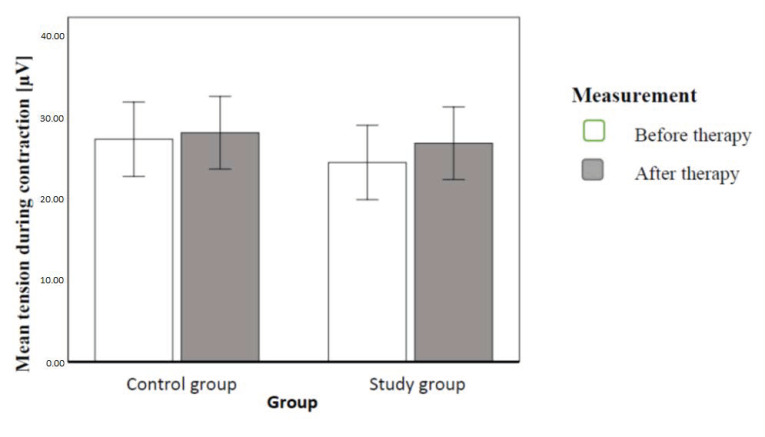
Results: In both groups, VRP (resting vaginal pressure) and resting PFM tension were significantly reduced. The strength and endurance of PFM, tension during MVC and VSP (intravaginal pressure during contraction) increased, with no difference between the groups. SUI decreased significantly, and quality of life improved significantly in both groups.
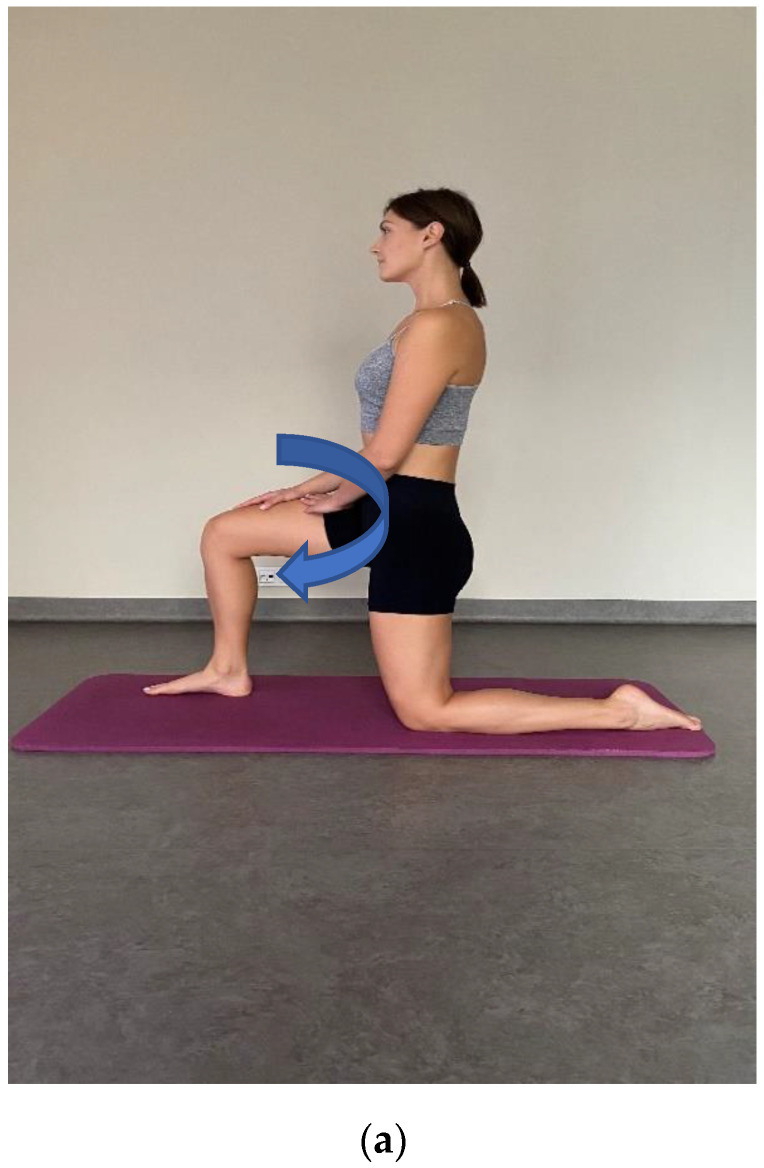
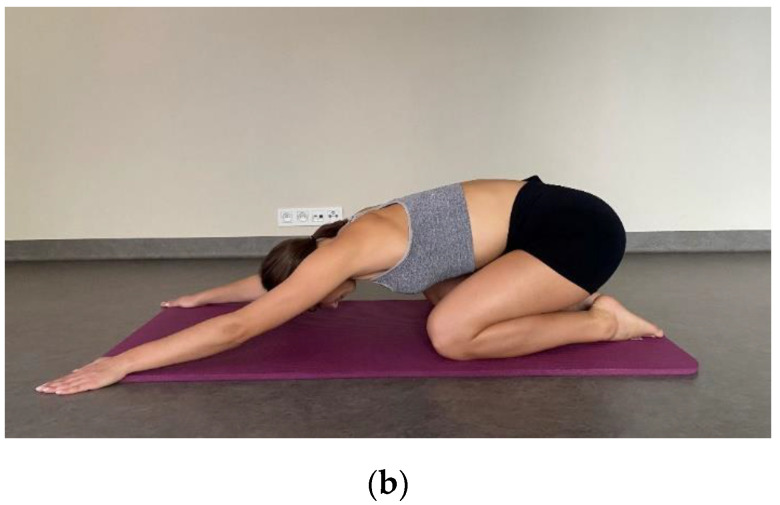
Conclusions: Education of the pelvic floor and changing habits significantly affected the activity of PFM and improved the quality of life in the group of patients with SUI. The posture correction therapy with manual therapy and stretching exercises did not increase this effect.
Keywords: body posture; corrective therapy; pelvic floor muscles; stress urinary incontinence.
Conflict of interest statement
Authors declare no conflict of interest.
Figures

References
-
- Comerford M., Mottram S. Kinetic Control–Ocena i Reedukacja Nieskoordynowanego Ruchu. Edra Urban & Partner; Wrocław, Poland: 2012.
-
- Gruszczyńska D., Dąbek A., Rekowski W. Diastasis recti abdominis–what may cause it in postpartum women? Adv. Rehabil. 2021;35:24–31. doi: 10.5114/areh.2021.103996. - DOI
-
- Hodges P.W., Sapsford R., Pangel H.M. Feedforward Activity of the Pelvic Floor Muscles Precedes Rapid Upper Limb Movements. Australian Physiotherapy Association; Melbourne, VIC, Australia: 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
