

Surgical and Oncological Outcomes of En-Bloc Resection for Malignancies Invading the Thoracic Spine
- PMID: 36614832
- PMCID: PMC9820992
- DOI: 10.3390/jcm12010031
Surgical and Oncological Outcomes of En-Bloc Resection for Malignancies Invading the Thoracic Spine
Abstract
Objective(s): There is still limited data in the literature concerning the survival of patients with tumors of the thoracic spine. In this study, we analyzed clinical features, perioperative and long-term outcomes in patients who underwent vertebrectomy for cancer. Furthermore, we evaluated the survival and surgical complications.
Methods: We retrospectively reviewed all cases of thoracic spinal tumors treated by the same team between 1998 and 2018. We divided them into three groups according to type of tumor (primary vertebral, primary lung and metastases) and compared outcomes. For each patient, Overall Survival (OS) and Cumulative Incidence of Relapse (CIR) were estimated. Complications and survival were analyzed using a logistic model.
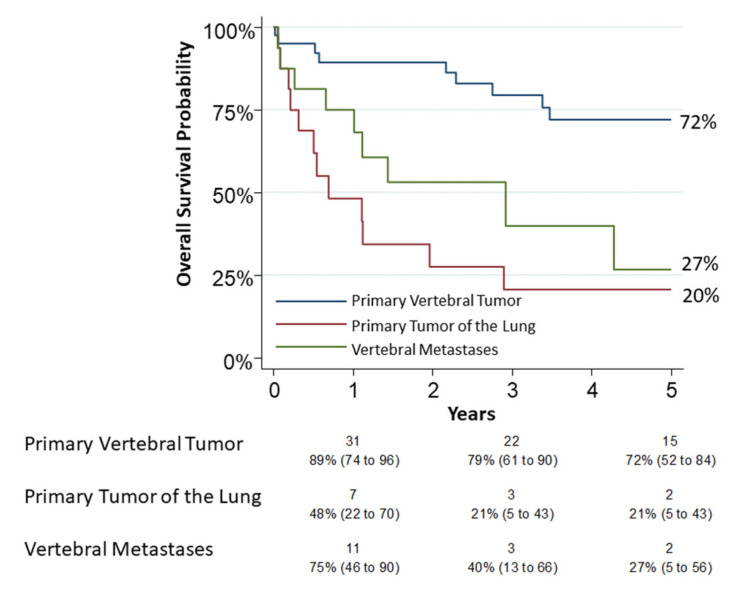
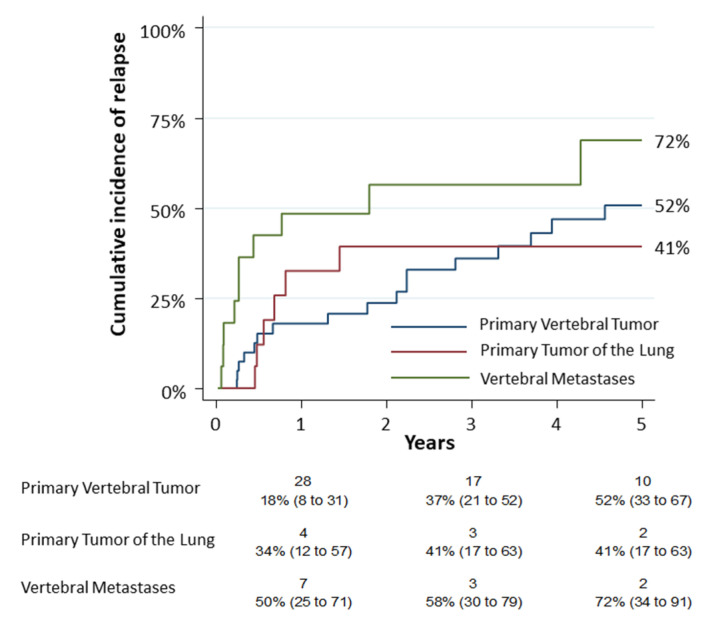
Results: Seventy-two patients underwent thoracic spine surgery (40 in group 1, 16 in each group 2 and 3). Thirty patients died at the end of the observation at a mean follow up time of 60 months (41%). The 5-year overall survival was 72% (95% CI: 0.52-0.84), 20% (95% CI: 0.05-0.43) and 27% (95% CI: 0.05-0.56) for each group, respectively. CIR of group 3 was higher (HR 2.57, 95% CI: 1.22-5.45, p = 0.013). The logistic model revealed that age was related to complications (p = 0.04), while surgery for a type 3 tumor was related to mortality (p = 0.02).
Conclusions: Although the cohort size was limited, primary vertebral tumors displayed the best 5-y-OS with an acceptable complications rate. The indication of surgery should be advised by a multidisciplinary team and only for selected cases. Finally, the use of a combined approach does not increase the risk of complications.
Keywords: lung cancer invading spine; spine tumor; vertebral T4 NSCLC; vertebral metastases; vertebral tumor resection.
Conflict of interest statement
Giulia Veronesi has received honoraria from AbMedica SpA, Medtronic and Johnson & Johnson. The other authors declare no conflicts of interest. This study did not receive funds. The other authors declare no conflict of interest.
Figures
References
-
- Pettiford B.L., Schuchert M.J., Jeyabalan G., Landreneau J.R., Kilic A., Landreneau J.P., Awais O., Kent M.S., Ferson P.F., Luketich J.D., et al. Technical challenges and utility of anterior exposure for thoracic spine pathology. Ann. Thorac. Surg. 2008;86:1762–1768. doi: 10.1016/j.athoracsur.2008.07.087. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
