

Which Surgery for Stage II-III Empyema Patients? Observational Single-Center Cohort Study of 719 Consecutive Patients
- PMID: 36614937
- PMCID: PMC9821231
- DOI: 10.3390/jcm12010136
Which Surgery for Stage II-III Empyema Patients? Observational Single-Center Cohort Study of 719 Consecutive Patients
Abstract
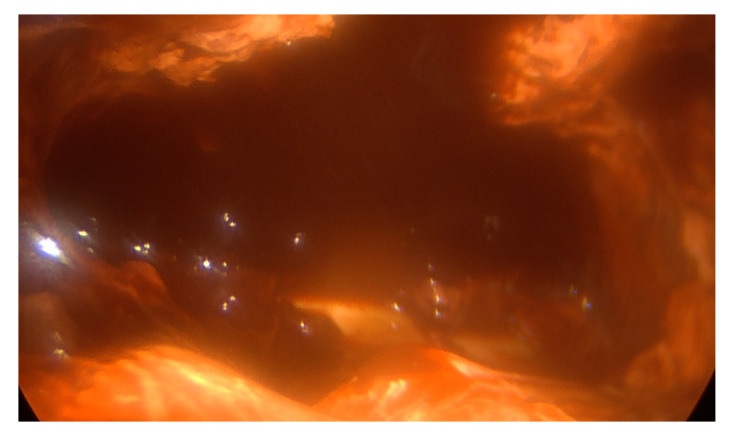
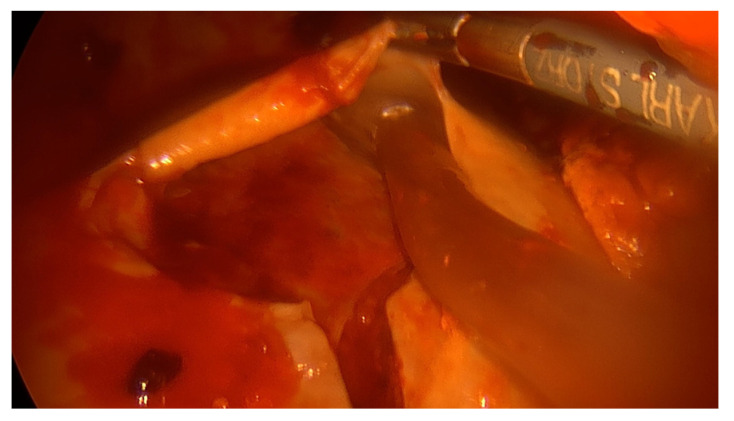
Objective: Recent guidelines support the use of thoracoscopic surgery in stage II-III empyema; however, there is still debate regarding the best surgical approach. The aim of our study is to compare postoperative outcomes of VATS and open surgical approaches for the treatment of post-pneumonic empyema.
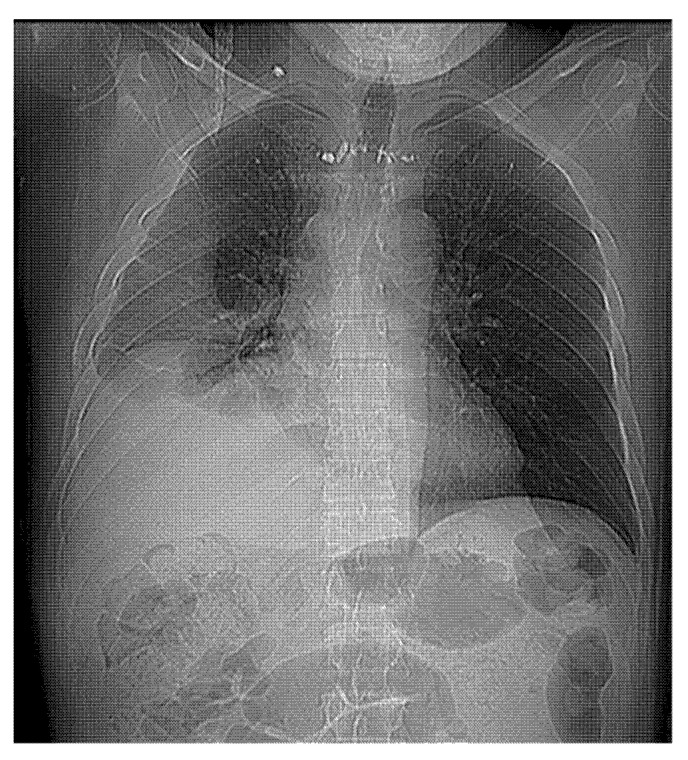
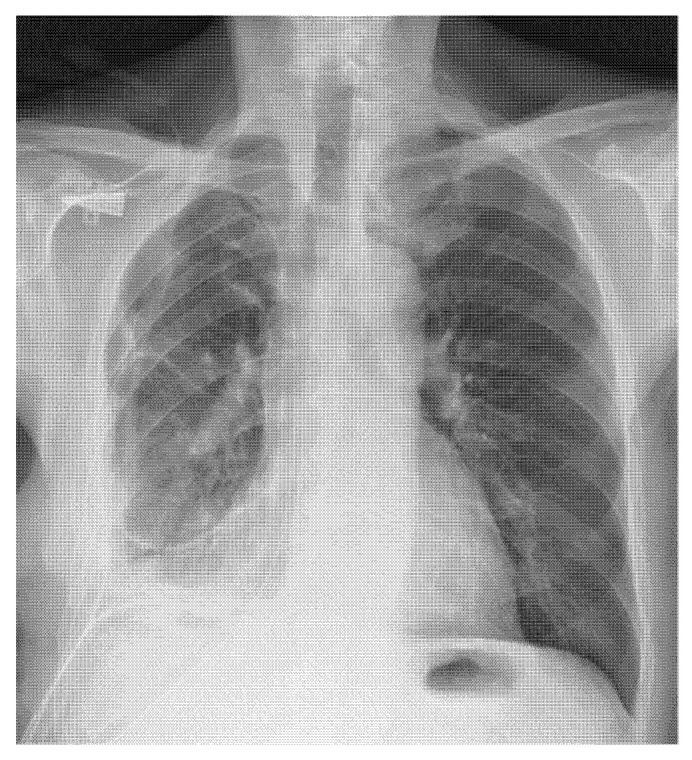
Methods: Observational cohort study on prospectively collected cases of post-pneumonic empyema surgically treated in a single center (2000-2020). Patients were divided into an open group (OT, posterolateral muscle sparing thoracotomy) and VATS group (VT, 2 or 3 port ± utility incision). The primary outcome of the study was empyema resolution, assessed by the recurrence rate. Secondary outcomes were mortality, complications, pain and return to daily life. All patients were followed up at 1, 3 and 6 months after surgery in the outpatient clinic with a chest radiograph/CT scan.
Results: In total, 719 consecutive patients were surgically treated for stage II-III empyema, with 644 belonging to the VT group and 75 to the OT group. All patients had a clinical history of pneumonia lasting no more than 6 months before surgery, and 553 (76.9%) had stage II empyema. Operative time was 92.7 ± 6.8 min for the OT group and 112.2 ± 7.4 for the VT group. The conversion rate was 8.4% (46/545) for stage II and 19.2% (19/99) for stage III. Twelve patients (1.86%) in the VT group and four patients (5.3%) in the OT group underwent additional surgery for bleeding. Postoperative mortality was 1.25% (9/719): 5.3% (4/75) in OT and 0.77% (5/644) in VT. Postoperative stay was 10 ± 6.5 days in OT and 8 ± 2.4 in VT. Overall morbidity was 14.7% (106/719): 21.3% (16/75) in OT and 13.9% (90/644) in VT. In VT, six patients (0.93%) showed recurrent empyema: five were treated with chest drainage and one with additional open surgery.
Conclusions: Our findings suggest that the VATS approach, showing a 99% success rate, shorter length of stay and lower postoperative morbidity, should be considered the treatment of choice for thoracic empyema.
Keywords: VATS; minimally invasive surgery; outcomes; pleural empyema; surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Dadonaite B., Roser M. Pneumonia. Our World in Data 2018. [(accessed on 13 August 2022)]. Available online: https://ourworldindata.org/pneumonia.
-
- Andrews N.C., Parker E.F., Shaw R.R., Wilson N.J., Webb W.R. Management of nontuberculous empyema. Am. Rev. Respir. Dis. 1962;85:935–936.
LinkOut - more resources
Full Text Sources
