

Peri-Procedural Troponin Elevation after Percutaneous Coronary Intervention for Left Main Coronary Artery Disease
- PMID: 36615044
- PMCID: PMC9821242
- DOI: 10.3390/jcm12010244
Peri-Procedural Troponin Elevation after Percutaneous Coronary Intervention for Left Main Coronary Artery Disease
Abstract
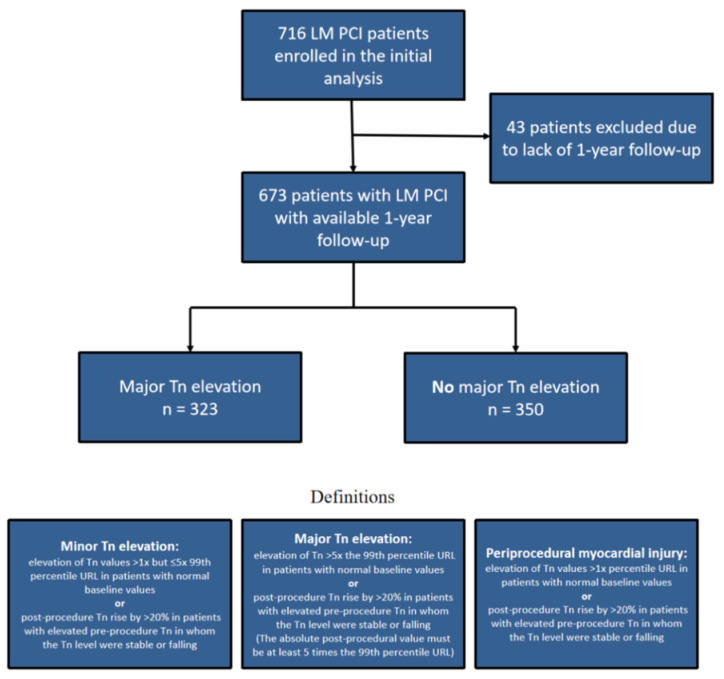
Left main (LM) percutaneous coronary interventions (PCI) are challenging and highly invasive procedures. Periprocedural myocardial injury (Troponin (Tn) elevation > 99th percentile) is frequently detected after LM PCI, being identified even in up to 67% of patients. However, the prognostic implications of periprocedural Tn elevation after LM PCI remain controversial. We aim to assess the impact and prognostic significance of the periprocedural troponin elevation on long-term outcomes in patients undergoing LM PCI in a real-world setting. Consecutive 673 patients who underwent LM PCI in our department between January 2015 to February 2021 were included in a prospective registry. The first group consisted of 323 patients with major cardiac Troponin I elevation defined as an elevation of Tn values > 5× the 99th percentile in patients with normal baseline values or post-procedure Tn rise by >20% in patients with elevated pre-procedure Tn in whom the Tn level was stable or falling (based on the fourth universal definition of myocardial infarction). The second group consisted of patients without major cardiac Troponin I elevation. Seven-year long-term all-cause mortality was not higher in the group with major Tn elevation (36.9% vs. 40.6%; p = 0.818). Naturally, periprocedural myocardial infarction was diagnosed only in patients from groups with major Tn elevation (4.9% of all patients). In-hospital death and other periprocedural complications did not differ significantly between the two study groups. The adjusted HRs for mortality post-PCI in patients with a periprocedural myocardial infarction were not significant. Long-term mortality subanalysis for the group with criteria for cardiac procedural myocardial injury showed no significant differences (39.5% vs. 38.8%; p = 0.997). The occurrence of Tn elevation (>1×; >5×; >35× and >70× URL) after LM PCI was not associated with adverse long-term outcomes. The results of the study suggest that the isolated periprocedural troponin elevation is not clinically significant.
Keywords: coronary artery disease; left main; percutaneous coronary intervention; periprocedural myocardial injury; troponin elevation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Implications of Periprocedural Myocardial Biomarker Elevations and Commonly Used MI Definitions After Left Main PCI.JACC Cardiovasc Interv. 2021 Aug 9;14(15):1623-1634. doi: 10.1016/j.jcin.2021.05.006. JACC Cardiovasc Interv. 2021. PMID: 34353593
-
Procedural myocardial injury, infarction and mortality in patients undergoing elective PCI: a pooled analysis of patient-level data.Eur Heart J. 2021 Jan 21;42(4):323-334. doi: 10.1093/eurheartj/ehaa885. Eur Heart J. 2021. PMID: 33257958 Free PMC article.
-
Prognostically relevant periprocedural myocardial injury and infarction associated with percutaneous coronary interventions: a Consensus Document of the ESC Working Group on Cellular Biology of the Heart and European Association of Percutaneous Cardiovascular Interventions (EAPCI).Eur Heart J. 2021 Jul 15;42(27):2630-2642. doi: 10.1093/eurheartj/ehab271. Eur Heart J. 2021. PMID: 34059914 Free PMC article.
-
The prognosis of periprocedural myocardial infarction after percutaneous coronary interventions.Cardiovasc Revasc Med. 2013 Jan-Feb;14(1):32-6. doi: 10.1016/j.carrev.2012.10.006. Epub 2012 Nov 17. Cardiovasc Revasc Med. 2013. PMID: 23164601 Review.
-
The clinical approach to diagnosing peri-procedural myocardial infarction after percutaneous coronary interventions according to the fourth universal definition of myocardial infarction - from the study group on biomarkers of the European Society of Cardiology (ESC) Association for Acute CardioVascular Care (ACVC).Biomarkers. 2022 Jul;27(5):407-417. doi: 10.1080/1354750X.2022.2055792. Epub 2022 May 26. Biomarkers. 2022. PMID: 35603440 Free PMC article. Review.
References
-
- Morice M.-C., Serruys P.W., Kappetein A.P., Feldman T.E., Stahle E., Colombo A., Mack M.J., Holmes D.R., Torracca L., van Es G.A., et al. Outcomes in patients with de novo left main disease treated with either percutaneous coronary intervention using paclitaxel-eluting stents or coronary artery bypass graft treatment in the Synergy Between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery (SYNTAX) trial. Circulation. 2010;121:2645–2653. - PubMed
-
- Park D.-W., Ahn J.-M., Park H., Yun S.-C., Kang D.-Y., Lee P.H., Kim Y.H., Lim D.S., Rha S.W., Park G.M., et al. Ten-Year Outcomes After Drug-Eluting Stents Versus Coronary Artery Bypass Grafting for Left Main Coronary Disease: Extended Follow-Up of the PRECOMBAT Trial. Circulation. 2020;141:1437–1446. doi: 10.1161/CIRCULATIONAHA.120.046039. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
