

Management of Hemorrhagic Shock: Physiology Approach, Timing and Strategies
- PMID: 36615060
- PMCID: PMC9821021
- DOI: 10.3390/jcm12010260
Management of Hemorrhagic Shock: Physiology Approach, Timing and Strategies
Abstract
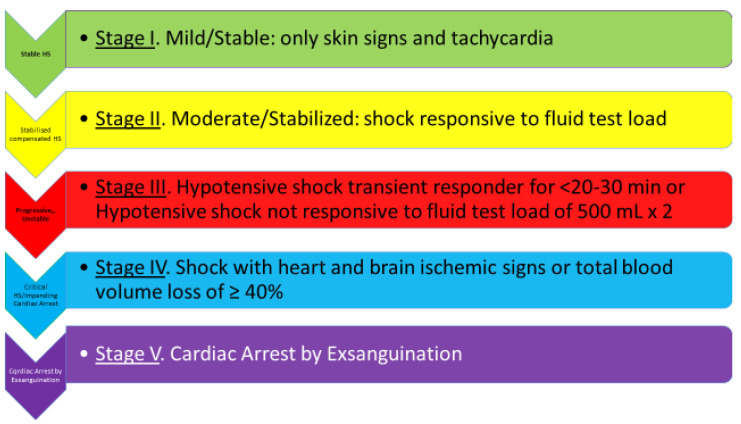
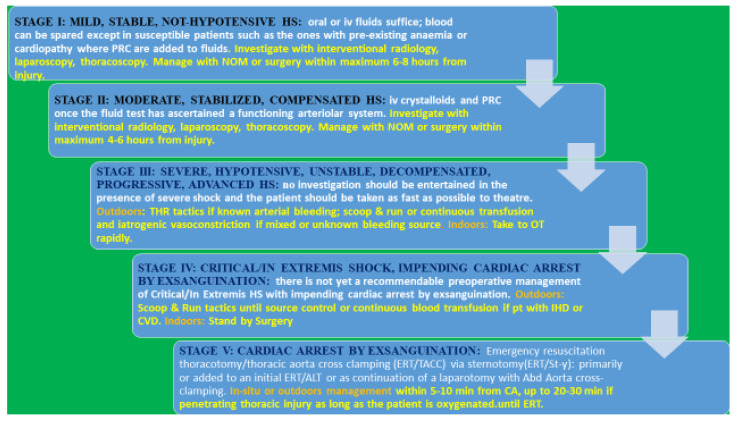
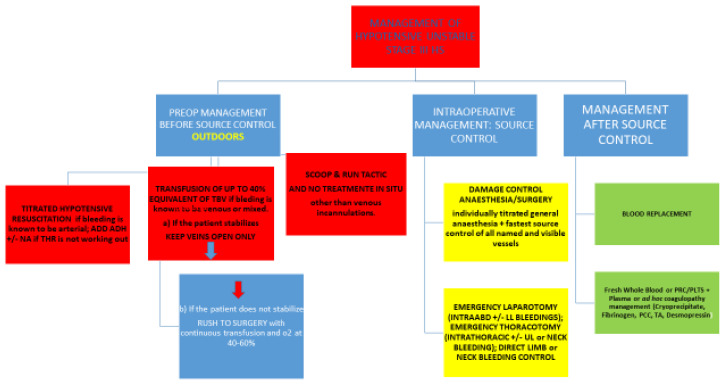
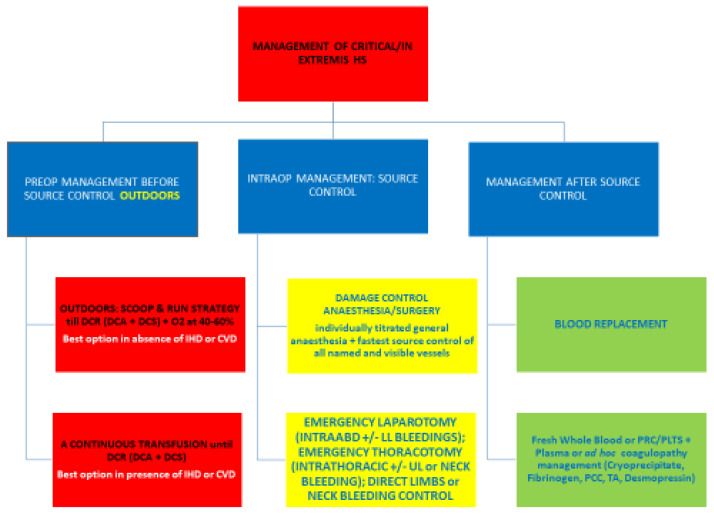
Hemorrhagic shock (HS) management is based on a timely, rapid, definitive source control of bleeding/s and on blood loss replacement. Stopping the hemorrhage from progressing from any named and visible vessel is the main stem fundamental praxis of efficacy and effectiveness and an essential, obligatory, life-saving step. Blood loss replacement serves the purpose of preventing ischemia/reperfusion toxemia and optimizing tissue oxygenation and microcirculation dynamics. The "physiological classification of HS" dictates the timely management and suits the 'titrated hypotensive resuscitation' tactics and the 'damage control surgery' strategy. In any hypotensive but not yet critical shock, the body's response to a fluid load test determines the cut-off point between compensation and progression between the time for adopting conservative treatment and preparing for surgery or rushing to the theater for rapid bleeding source control. Up to 20% of the total blood volume is given to refill the unstressed venous return volume. In any critical level of shock where, ab initio, the patient manifests signs indicating critical physiology and impending cardiac arrest or cardiovascular accident, the balance between the life-saving reflexes stretched to the maximum and the insufficient distal perfusion (blood, oxygen, and substrates) remains in a liable and delicate equilibrium, susceptible to any minimal change or interfering variable. In a cardiac arrest by exsanguination, the core of the physiological issue remains the rapid restoration of a sufficient venous return, allowing the heart to pump it back into systemic circulation either by open massage via sternotomy or anterolateral thoracotomy or spontaneously after aorta clamping in the chest or in the abdomen at the epigastrium under extracorporeal resuscitation and induced hypothermia. This is the only way to prevent ischemic damage to the brain and the heart. This is accomplishable rapidly and efficiently only by a direct approach, which is a crush laparotomy if the bleeding is coming from an abdominal +/- lower limb site or rapid sternotomy/anterolateral thoracotomy if the bleeding is coming from a chest +/- upper limbs site. Without first stopping the bleeding and refilling the heart, any further exercise is doomed to failure. Direct source control via laparotomy/thoracotomy, with the concomitant or soon following venous refilling, are the two essential, initial life-saving steps.
Keywords: damage control surgery; exsanguination; fluid load test; hemorrhagic shock; hypotensive resuscitation; titrated-to-response anesthesia.
Conflict of interest statement
The author declares no conflict of interest.
Figures
Similar articles
-
The Need for a Physiological Classification of Hemorrhagic Shock.J Emerg Trauma Shock. 2020 Jul-Sep;13(3):177-182. doi: 10.4103/JETS.JETS_153_19. Epub 2020 Sep 18. J Emerg Trauma Shock. 2020. PMID: 33304066 Free PMC article. Review.
-
Use of an intravascular temperature control catheter for rewarming of hypothermic trauma patients with ongoing hemorrhagic shock after combined damage control thoracotomy and laparotomy: A case series.Injury. 2018 Sep;49(9):1668-1674. doi: 10.1016/j.injury.2018.07.008. Epub 2018 Jul 8. Injury. 2018. PMID: 30017181
-
Chest compression-related fatal internal mammary artery injuries manifesting after venoarterial extracorporeal membrane oxygenation: a case series.J Med Case Rep. 2017 Nov 11;11(1):318. doi: 10.1186/s13256-017-1485-y. J Med Case Rep. 2017. PMID: 29126457 Free PMC article.
-
[Comments on the 2010 guidelines on cardiopulmonary resuscitation of the European Resuscitation Council].Anaesthesist. 2010 Dec;59(12):1105-23. doi: 10.1007/s00101-010-1820-9. Anaesthesist. 2010. PMID: 21125214 German.
-
Exsanguination in trauma: A review of diagnostics and treatment options.Injury. 2009 Jan;40(1):11-20. doi: 10.1016/j.injury.2008.10.007. Epub 2009 Jan 8. Injury. 2009. PMID: 19135193 Review.
Cited by
-
Navigating Hemorrhagic Shock: Biomarkers, Therapies, and Challenges in Clinical Care.Biomedicines. 2024 Dec 17;12(12):2864. doi: 10.3390/biomedicines12122864. Biomedicines. 2024. PMID: 39767770 Free PMC article. Review.
-
Comparing the effect of pre-anesthesia clonidine and tranexamic acid on intraoperative bleeding volume in rhinoplasty: a machine learning approach.Sci Rep. 2025 Aug 17;15(1):30062. doi: 10.1038/s41598-025-07450-3. Sci Rep. 2025. PMID: 40820015 Free PMC article.
-
Can a breast hematoma lead to hemorrhagic shock in elderly trauma patients with multiple comorbidities and reduced physiological reserve? Examining the risks and management strategies.Radiol Case Rep. 2024 Oct 26;20(1):314-319. doi: 10.1016/j.radcr.2024.10.011. eCollection 2025 Jan. Radiol Case Rep. 2024. PMID: 39539386 Free PMC article.
-
Electrospun Silk-ICG Composite Fibers and the Application toward Hemorrhage Control.J Funct Biomater. 2024 Sep 19;15(9):272. doi: 10.3390/jfb15090272. J Funct Biomater. 2024. PMID: 39330247 Free PMC article.
-
Echocardiography as a Vital Tool in Assessing Shock: A Comprehensive Review.Cureus. 2024 Mar 31;16(3):e57310. doi: 10.7759/cureus.57310. eCollection 2024 Mar. Cureus. 2024. PMID: 38690492 Free PMC article. Review.
References
-
- Tiba M.H., Awad A.B., Pennington A., Fung C.M., Napolitano L.M., Park P.K., Machado-Aranda D.A., Gunnerson K.J., Romfh P., Ward K.R. Resonance Raman Spectroscopy Derived Tissue Hemoglobin Oxygen Saturation in Critically Ill and Injured Patients. Shock. 2020;56:92–97. doi: 10.1097/SHK.0000000000001696. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
