

Ethnic differences in COVID-19 mortality in the second and third waves of the pandemic in England during the vaccine rollout: a retrospective, population-based cohort study
- PMID: 36617562
- PMCID: PMC9826727
- DOI: 10.1186/s12916-022-02704-7
Ethnic differences in COVID-19 mortality in the second and third waves of the pandemic in England during the vaccine rollout: a retrospective, population-based cohort study
Abstract
Background: Ethnic minority groups in England have been disproportionately affected by the COVID-19 pandemic and have lower vaccination rates than the White British population. We examined whether ethnic differences in COVID-19 mortality in England have continued since the vaccine rollout and to what extent differences in vaccination rates contributed to excess COVID-19 mortality after accounting for other risk factors.
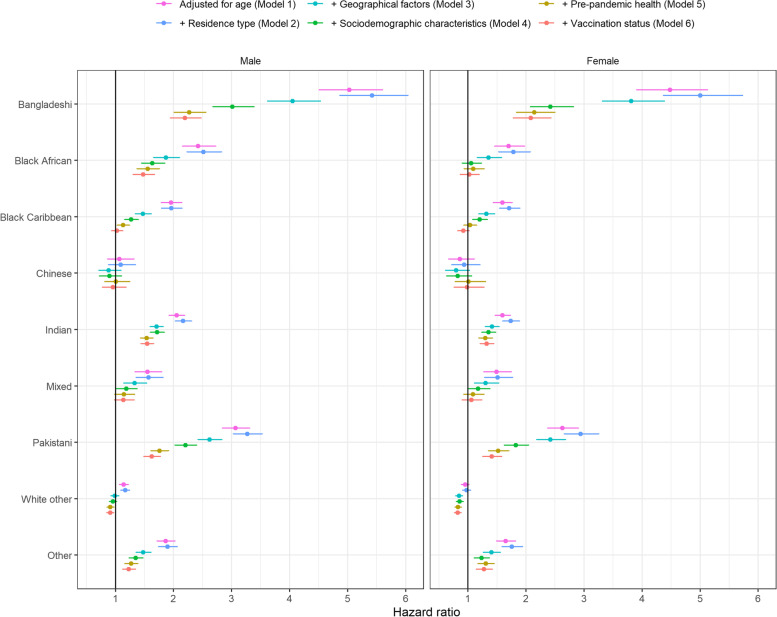
Methods: We conducted a retrospective, population-based cohort study of 28.8 million adults aged 30-100 years in England. Self-reported ethnicity was obtained from the 2011 Census. The outcome was death involving COVID-19 during the second (8 December 2020 to 12 June 2021) and third wave (13 June 2021 to 1 December 2021). We calculated hazard ratios (HRs) for death involving COVID-19, sequentially adjusting for age, residence type, geographical factors, sociodemographic characteristics, pre-pandemic health, and vaccination status.
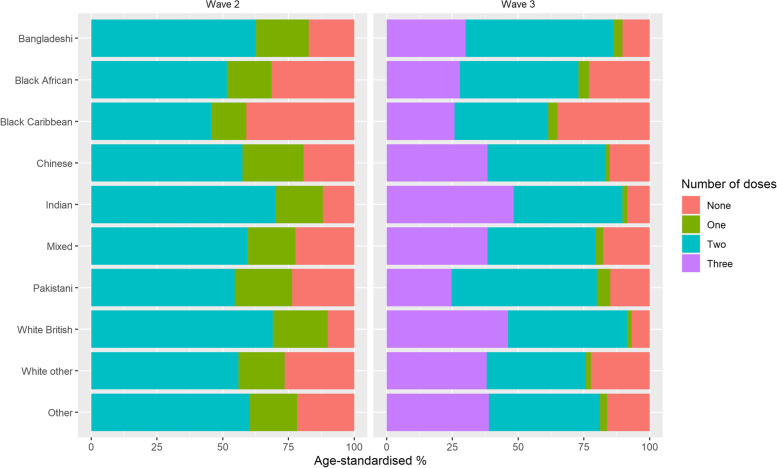
Results: Age-adjusted HRs of death involving COVID-19 were elevated for most ethnic minority groups during both waves, particularly for groups with lowest vaccination rates (Bangladeshi, Pakistani, Black African, and Black Caribbean). HRs were attenuated after adjusting for geographical factors, sociodemographic characteristics, and pre-pandemic health. Further adjusting for vaccination status substantially reduced residual HRs for Black African, Black Caribbean, and Pakistani groups in the third wave. Fully adjusted HRs only remained elevated for the Bangladeshi group (men: 2.19 [95% CI 1.72-2.78]; women: 2.12 [1.58-2.86]) and Pakistani men (1.24 [1.06-1.46]).
Conclusions: Lower COVID-19 vaccination uptake in several ethnic minority groups may drive some of the differences in COVID-19 mortality compared to White British. Public health strategies to increase vaccination uptake in ethnic minority groups would help reduce inequalities in COVID-19 mortality, which have remained substantial since the start of the vaccination campaign.
Keywords: COVID-19; Coronavirus; Ethnic group; Ethnicity; Mortality; SARS-CoV-2; Vaccination.
© 2023. Crown.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures


References
-
- Mathur R, Rentsch CT, Morton CE, Hulme WJ, Schultze A, MacKenna B, et al. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform. Lancet. 2021;397:1711–1724. doi: 10.1016/S0140-6736(21)00634-6. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
