

Imaging subclinical coronary atherosclerosis to guide lipid management, are we there yet?
- PMID: 36619296
- PMCID: PMC9813535
- DOI: 10.1016/j.ajpc.2022.100451
Imaging subclinical coronary atherosclerosis to guide lipid management, are we there yet?
Abstract
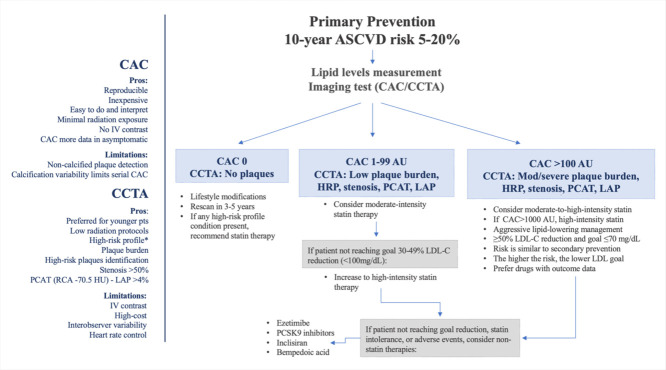
Atherosclerotic cardiovascular disease risk (ASCVD) is an ongoing epidemic, and lipid abnormalities are its primordial cause. Most individuals suffering a first ASCVD event are previously asymptomatic and often do not receive preventative therapies. The cornerstone of primary prevention has been the identification of individuals at risk through risk calculators based on clinical and laboratory traditional risk factors plus risk enhancers. However, it is well accepted that a clinical risk calculator misclassifies a significant proportion of individuals leading to the prescription of a lipid-lowering medication with very little yield or a missed opportunity for lipid-lowering agents with a potentially preventable event. The development of coronary artery calcium scoring (CAC) and CT coronary angiography (CCTA) provide complementary tools to directly visualize coronary plaque and other risk-modifying imaging components that can potentially provide individualized lipid management. Understanding patient selection for CAC or potentially CCTA and the risk implications of the different parameters provided, such as CAC score, coronary stenosis, plaque characteristics and burden, epicardial adipose tissue, and pericoronary adipose tissue, have grown more complex as technologies evolve. These parameters directly affect the shared decision with patients to start or withhold lipid-lowering therapies, to adjust statin intensity or LDL cholesterol goals. Emerging lipid lowering studies with non-invasive imaging as a guide to patient selection and treatment efficacy, plus the evolution of lipid lowering therapies from statins to a diverse armament of newer high-cost agents have pushed these two fields forward with a complex interaction. This review will discuss existing risk estimators, and non-invasive imaging techniques for subclinical coronary atherosclerosis, traditionally studied using CAC and more recently CCTA with qualitative and quantitative measurements. We will also explore the current data, gaps of knowledge and future directions on the use of these techniques in the risk-stratification and guidance of lipid management.
Keywords: CAC; CCTA; Lipids; Plaque burden; Plaque characterization.
© 2022 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Arnett DK, Blumenthal RS, Albert MA, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;140(11):e596–e646. doi: 10.1161/CIR.0000000000000678. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
