

Continuous population-level monitoring of SARS-CoV-2 seroprevalence in a large European metropolitan region
- PMID: 36619367
- PMCID: PMC9811913
- DOI: 10.1016/j.isci.2023.105928
Continuous population-level monitoring of SARS-CoV-2 seroprevalence in a large European metropolitan region
Abstract
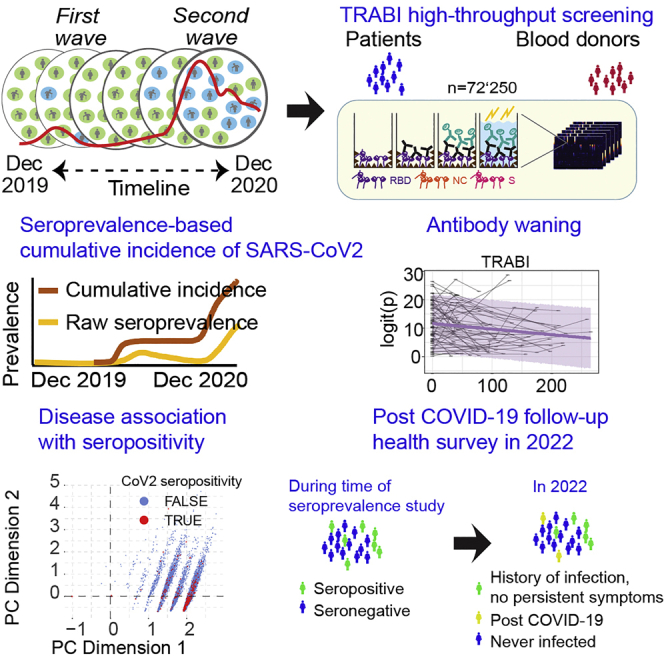
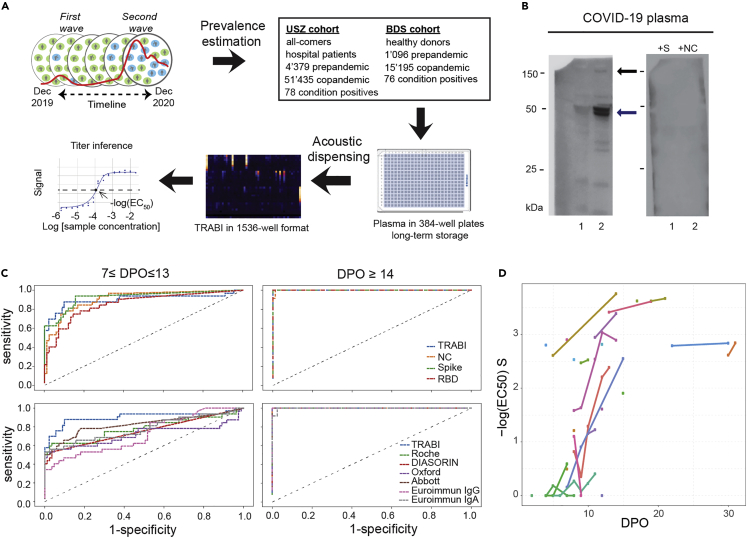
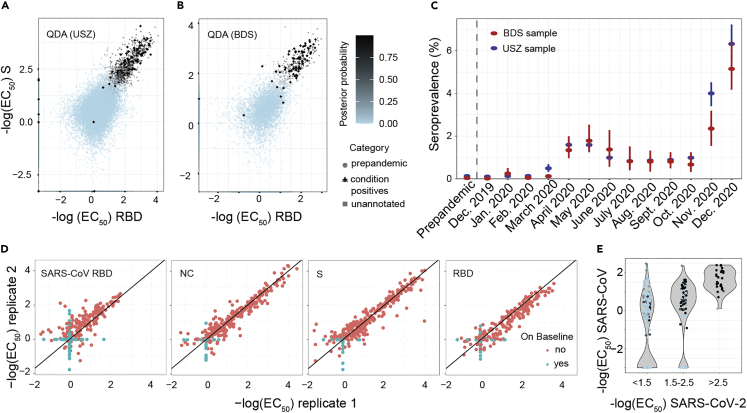
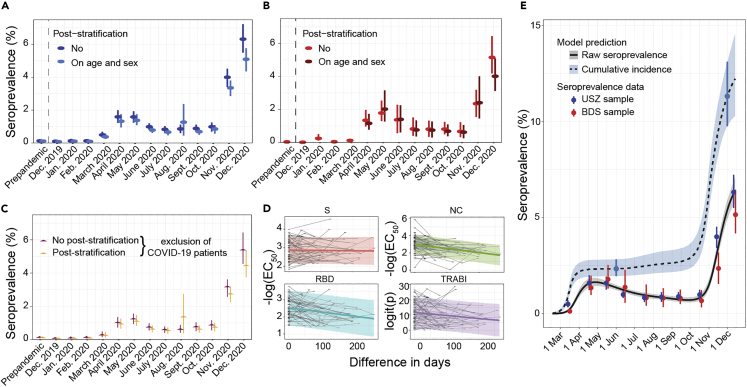
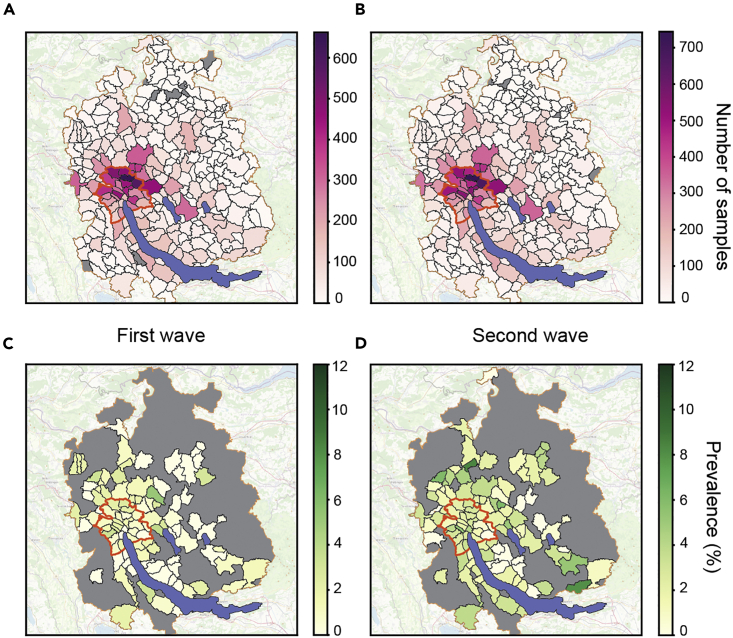
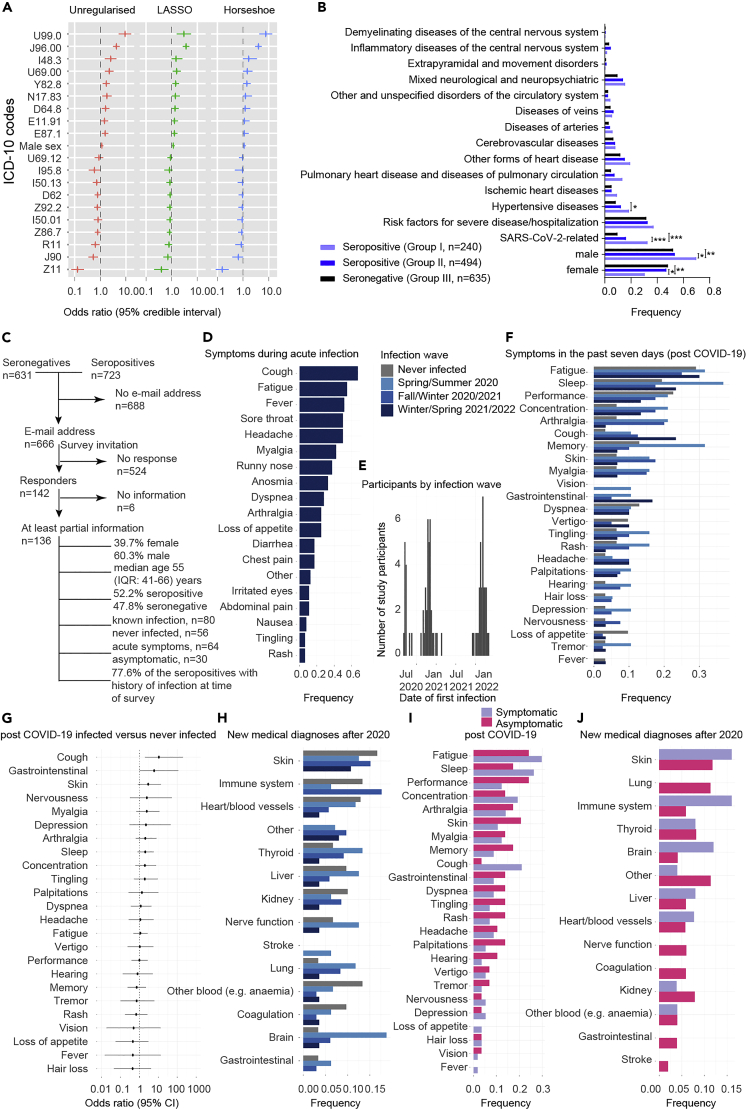
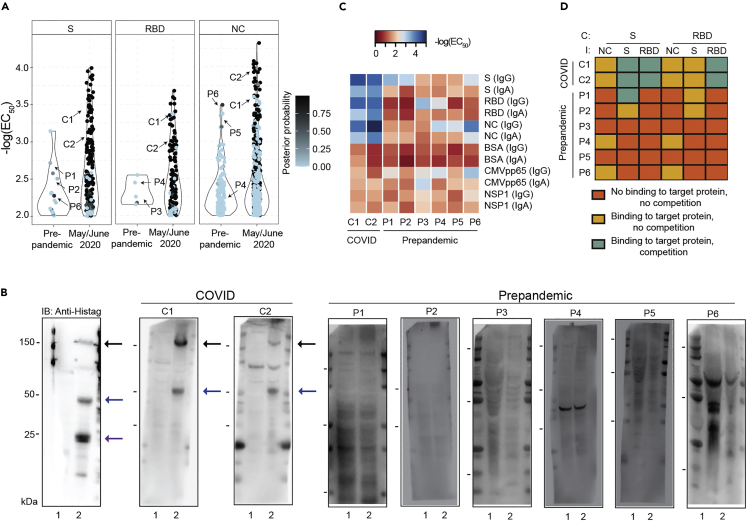
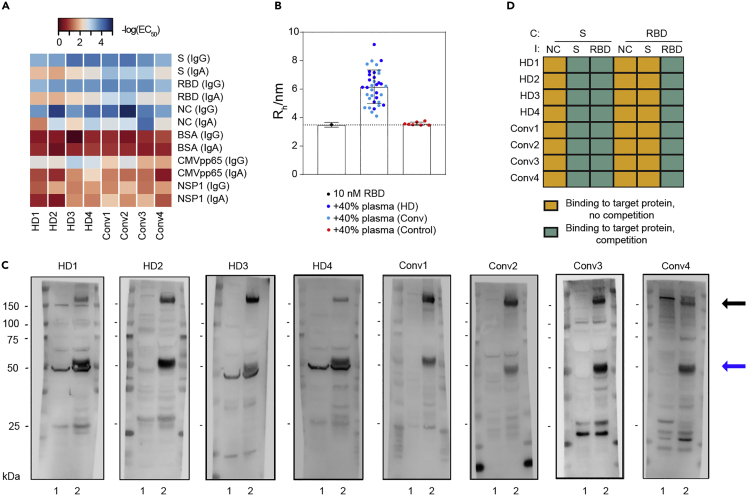
Effective public health measures against SARS-CoV-2 require granular knowledge of population-level immune responses. We developed a Tripartite Automated Blood Immunoassay (TRABI) to assess the IgG response against three SARS-CoV-2 proteins. We used TRABI for continuous seromonitoring of hospital patients and blood donors (n = 72'250) in the canton of Zurich from December 2019 to December 2020 (pre-vaccine period). We found that antibodies waned with a half-life of 75 days, whereas the cumulative incidence rose from 2.3% in June 2020 to 12.2% in mid-December 2020. A follow-up health survey indicated that about 10% of patients infected with wildtype SARS-CoV-2 sustained some symptoms at least twelve months post COVID-19. Crucially, we found no evidence of a difference in long-term complications between those whose infection was symptomatic and those with asymptomatic acute infection. The cohort of asymptomatic SARS-CoV-2-infected subjects represents a resource for the study of chronic and possibly unexpected sequelae.
Keywords: Biological database; Immunology; Microbiology; Virology.
© 2023 The Authors.
Conflict of interest statement
TPJK is a member of the board of directors of Fluidic Analytics. AA is a member of the board of directors of Mabylon AG which has funded antibody-related work in the Aguzzi lab in the past. All other authors declare no competing interests.
Figures
References
-
- Lamparter, D., Jacquat, R.P.B., Riou, J., Menges, D., Ballouz, T., and Emmenegger, M. (2022). Code repository for SARS-CoV-2 seroprevalence study. 10.5281/ZENODO.7454292.
-
- Statistisches Amt Kanton Zuerich Open ZH github. 2020. https://github.com/openZH/covid_19
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
