

Effect of prehospital transportation on 24-h fluid volume, a post hoc analysis of a multicenter, prospective, observational study on fluid volumes in patients with suspected infection
- PMID: 36619623
- PMCID: PMC9810619
- DOI: 10.3389/fmed.2022.1052071
Effect of prehospital transportation on 24-h fluid volume, a post hoc analysis of a multicenter, prospective, observational study on fluid volumes in patients with suspected infection
Abstract
Introduction: Infections, including sepsis, are leading causes of death and fluid administration is part of the treatment. The optimal fluid therapy remains controversial. If the patient is transported by Emergency Medical Services (EMS), fluids can be initiated during transportation, which may result in increased overall fluid administration and fluid overload, which may be harmful. The aim of the study was to investigate the effect of EMS transportation on 24-h fluid administration in patients with suspected infection.
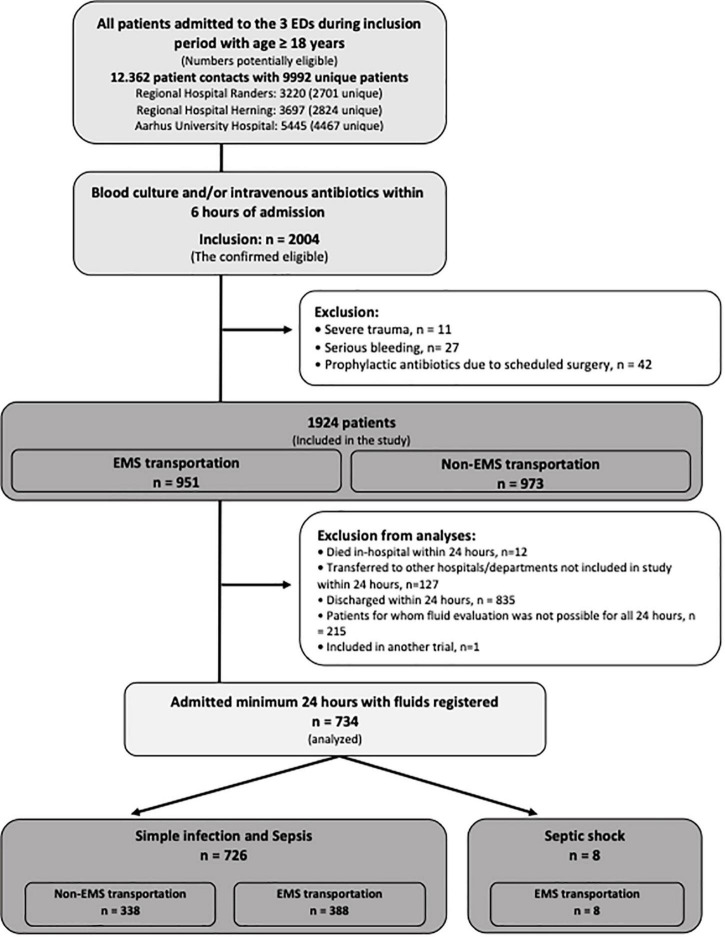
Methods: This is a post hoc study of a prospective, multicenter, observational study, conducted in three Danish Emergency Departments (EDs), 20 January-2 March 2020, aiming at describing fluid administration in patients with suspected infection. Patients were stratified into the groups: simple infection or sepsis, in accordance with SEPSIS-3-guidelines. The primary outcome of the current study was 24-h total fluid volume (oral and intravenous) stratified by transportation mode to the EDs.
Main results: Total 24-h fluids were registered for 734 patients. Patients with simple infection or sepsis arriving by EMS (n = 388, 54%) received mean 3,774 ml (standard deviation [SD]: 1900) and non-EMS received 3,627 ml (SD: 1568); mean difference (MD) was 303 ml [95% CI: 32; 573] adjusted for age, site, and total SOFA-score. Patients brought in by EMS received more intravenous fluids (MD: 621 ml [95% CI: 378; 864]) and less oral fluids (MD: -474 ml [95% CI: -616; -333]) than non-EMS patients.
Conclusion: Patients transported by EMS received more intravenous fluids and less oral fluids but overall, more fluid in total in the first 24-h than non-EMS after adjusting for age, site and SOFA-score.
Keywords: Emergency Medical Services (EMS); emergency department; fluid therapy; infection; sepsis.
Copyright © 2022 Jensen, Kølsen-Petersen, Kirkegaard and Jessen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Twenty-four-hour fluid administration in emergency department patients with suspected infection: A multicenter, prospective, observational study.Acta Anaesthesiol Scand. 2021 Sep;65(8):1122-1142. doi: 10.1111/aas.13848. Epub 2021 May 18. Acta Anaesthesiol Scand. 2021. PMID: 33964019
-
Effect of Out-Of-Hour Admission on Fluid Treatment of Emergency Department Patients with Suspected Infection; a Multicenter Post-Hoc Analysis.Arch Acad Emerg Med. 2023 Jan 31;11(1):e21. doi: 10.22037/aaem.v11i1.1839. eCollection 2023. Arch Acad Emerg Med. 2023. PMID: 36919142 Free PMC article.
-
Effectiveness of a Novel Rapid Infusion Device and Clinician Education for Early Fluid Therapy by Emergency Medical Services in Sepsis Patients: A Pre-Post Observational Study.Prehosp Emerg Care. 2024;28(6):753-760. doi: 10.1080/10903127.2023.2286292. Epub 2023 Dec 11. Prehosp Emerg Care. 2024. PMID: 38015064
-
Tricyclic antidepressant poisoning: an evidence-based consensus guideline for out-of-hospital management.Clin Toxicol (Phila). 2007;45(3):203-33. doi: 10.1080/15563650701226192. Clin Toxicol (Phila). 2007. PMID: 17453872
-
Prehospital Sepsis Care.Emerg Med Clin North Am. 2017 Feb;35(1):175-183. doi: 10.1016/j.emc.2016.08.009. Emerg Med Clin North Am. 2017. PMID: 27908332 Review.
Cited by
-
Sepsis management in pre-hospital care - the earlier, the better?BMC Emerg Med. 2024 Nov 19;24(1):220. doi: 10.1186/s12873-024-01137-0. BMC Emerg Med. 2024. PMID: 39563231 Free PMC article.
References
LinkOut - more resources
Full Text Sources