

A case of clinical worsening after stereo-electroencephalographic-guided radiofrequency thermocoagulation in a patient with polymicrogyria
- PMID: 36620478
- PMCID: PMC9813673
- DOI: 10.1016/j.ebr.2022.100579
A case of clinical worsening after stereo-electroencephalographic-guided radiofrequency thermocoagulation in a patient with polymicrogyria
Abstract
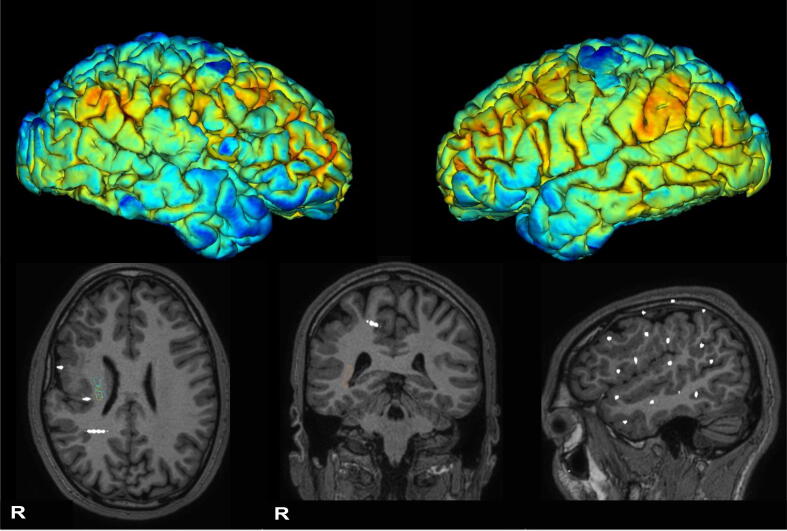
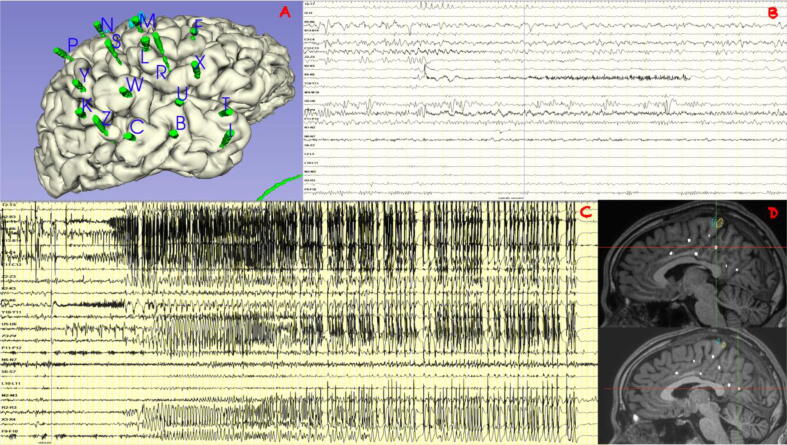
Radiofrequency thermocoagulation (RF-TC) is a wide-used procedure for drug-resistant epilepsy. The technique is considered safe with an overall risk of 1.1% of permanent complications, mainly focal neurological deficits. We report the case of a patient with drug-resistant epilepsy who complained of immediate seizure worsening and an unexpected event seven months following RF-TC. A 35-year-old male with drug-resistant epilepsy from the age of 18 years underwent stereoelectroencephalography (SEEG) implantation for a right peri-silvian polymicrogyria. He was excluded from surgery due to extent of the epileptogenic zone and the risk of visual field deficits. RF-TC was attempted to ablate the most epileptogenic zone identified by SEEG. After RF-TC, the patient reported an increase in seizure severity/frequency and experienced episodes of postictal psychosis. Off-label cannabidiol treatment led to improved seizure control and resolution of postictal psychosis. Patients with polymicrogyria (PwP) may present with a disruption of normal anatomy and the co-existence between epileptogenic zone and eloquent cortex within the malformation. RF-TC should be considered in PwP when they are excluded from surgery for prognostic and palliative purposes. However, given the complex interplay between pathological and electrophysiological networks in these patients, the remote possibility of clinical exacerbation after RF-TC should also be taken into account.
Keywords: CBD, Cannabidiol; Cannabidiol; EEG, electroencephalography; EZ, Epileptogenic Zone; Epilepsy; FDG-PET, Fluorodeoxyglucose-Positron Emission Tomography; Post-ictal psychosis; PwP, Patients with polymicrogyria; RF-TC, Radiofrequency thermocoagulation; Radiofrequency thermocoagulation; SEEG, stereo-electroencephalography; Stereo-EEG.
© 2022 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Stereoelectroencephalography-guided radiofrequency thermocoagulation in the epileptogenic zone: a retrospective study on 89 cases.J Neurosurg. 2015 Dec;123(6):1358-67. doi: 10.3171/2014.12.JNS141968. Epub 2015 Jun 19. J Neurosurg. 2015. PMID: 26090841
-
Stereo electroencephalography-guided radiofrequency thermocoagulation (SEEG-guided RF-TC) in drug-resistant focal epilepsy: Results from a 10-year experience.Epilepsia. 2017 Jan;58(1):85-93. doi: 10.1111/epi.13616. Epub 2016 Nov 16. Epilepsia. 2017. PMID: 27859033
-
Stereoelectroencephalography-guided radiofrequency thermocoagulation in drug-resistant focal epilepsy.Ann Transl Med. 2022 Feb;10(4):192. doi: 10.21037/atm-21-6851. Ann Transl Med. 2022. PMID: 35280357 Free PMC article.
-
Optimized stereoelectroencephalography-guided radiofrequency thermocoagulation in the treatment of patients with focal epilepsy.Ann Transl Med. 2020 Jan;8(1):15. doi: 10.21037/atm.2019.10.112. Ann Transl Med. 2020. PMID: 32055606 Free PMC article. Review.
-
Stereo-EEG-guided radiofrequency thermocoagulations.Epilepsia. 2017 Apr;58 Suppl 1:66-72. doi: 10.1111/epi.13687. Epilepsia. 2017. PMID: 28386919 Review.
References
-
- Rugg-Gunn F, Miserocchi A, McEvoy A. Epilepsy surgery. Pract Neurol. 2019 practneurol-2019-002192. https://doi.org/10.1136/practneurol-2019-002192. - PubMed
-
- West S., Nolan S.J., Newton R. Surgery for epilepsy: A systematic review of current evidence. Epileptic Disord. 2016;18(2):113–121. - PubMed
-
- Isnard J., Taussig D., Bartolomei F., Bourdillon P., Catenoix H., Chassoux F., et al. French guidelines on stereoelectroencephalography (SEEG) Neurophysiol Clin. 2018;48(1):5–13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources