Femoral impingement in maximal hip flexion is anterior-inferior distal to the cam deformity in femoroacetabular impingement patients with femoral retroversion : implications for hip arthroscopy
- PMID: 36620909
- PMCID: PMC9872041
- DOI: 10.1302/2046-3758.121.BJR-2022-0263.R1
Femoral impingement in maximal hip flexion is anterior-inferior distal to the cam deformity in femoroacetabular impingement patients with femoral retroversion : implications for hip arthroscopy
Abstract
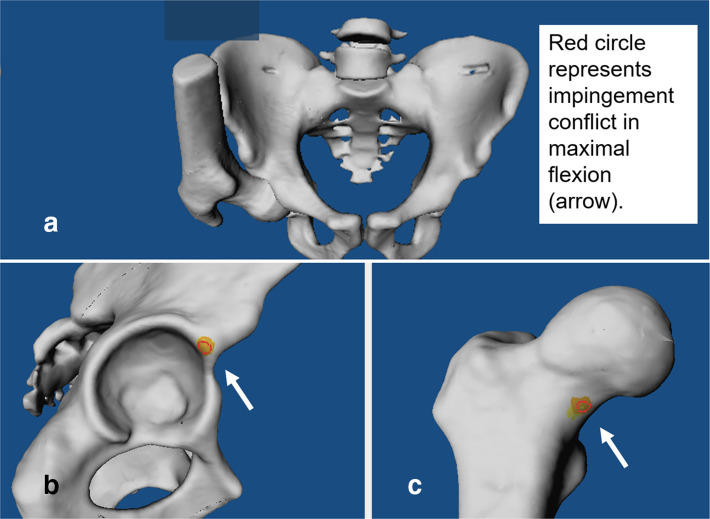
Aims: Femoroacetabular impingement (FAI) patients report exacerbation of hip pain in deep flexion. However, the exact impingement location in deep flexion is unknown. The aim was to investigate impingement-free maximal flexion, impingement location, and if cam deformity causes hip impingement in flexion in FAI patients.
Methods: A retrospective study involving 24 patients (37 hips) with FAI and femoral retroversion (femoral version (FV) < 5° per Murphy method) was performed. All patients were symptomatic (mean age 28 years (SD 9)) and had anterior hip/groin pain and a positive anterior impingement test. Cam- and pincer-type subgroups were analyzed. Patients were compared to an asymptomatic control group (26 hips). All patients underwent pelvic CT scans to generate personalized CT-based 3D models and validated software for patient-specific impingement simulation (equidistant method).
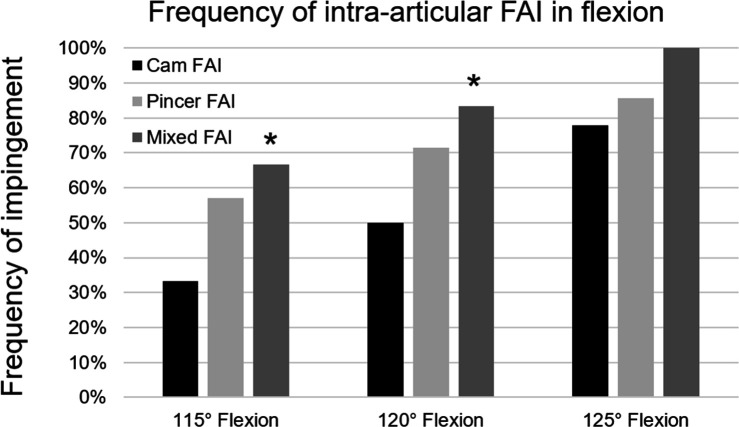
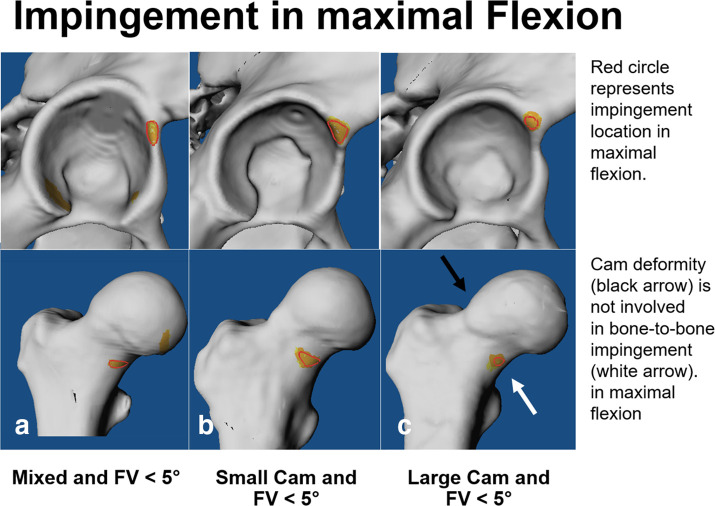
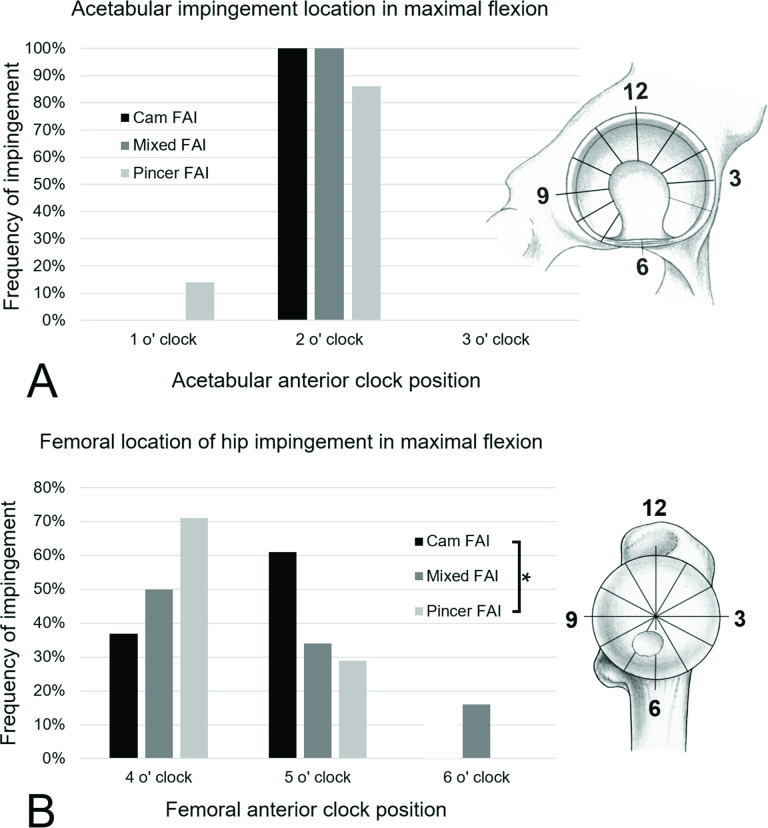
Results: Mean impingement-free flexion of patients with mixed-type FAI (110° (SD 8°)) and patients with pincer-type FAI (112° (SD 8°)) was significantly (p < 0.001) lower compared to the control group (125° (SD 13°)). The frequency of extra-articular subspine impingement was significantly (p < 0.001) increased in patients with pincer-type FAI (57%) compared to cam-type FAI (22%) in 125° flexion. Bony impingement in maximal flexion was located anterior-inferior at femoral four and five o'clock position in patients with cam-type FAI (63% (10 of 16 hips) and 37% (6 of 10 hips)), and did not involve the cam deformity. The cam deformity did not cause impingement in maximal flexion.
Conclusion: Femoral impingement in maximal flexion was located anterior-inferior distal to the cam deformity. This differs to previous studies, a finding which could be important for FAI patients in order to avoid exacerbation of hip pain in deep flexion (e.g. during squats) and for hip arthroscopy (hip-preservation surgery) for planning of bone resection. Hip impingement in flexion has implications for daily activities (e.g. putting on shoes), sports, and sex.Cite this article: Bone Joint Res 2023;12(1):22-32.
Keywords: CT scans; Extra-articular hip impingement; FAI; Femoroacetabular impingement; Hip arthroscopy; Hip preservation surgery; Subspine impingement; cam deformities; cam-type femoroacetabular impingement; femoral retroversion; femoroacetabular impingement; flexion; hip arthroscopy; hip flexion; hip pain; hips.
Figures