

Phenotypic and Genetic Factors Associated with Absence of Cardiomyopathy Symptoms in PLN:c.40_42delAGA Carriers
- PMID: 36622581
- PMCID: PMC10721704
- DOI: 10.1007/s12265-022-10347-5
Phenotypic and Genetic Factors Associated with Absence of Cardiomyopathy Symptoms in PLN:c.40_42delAGA Carriers
Abstract
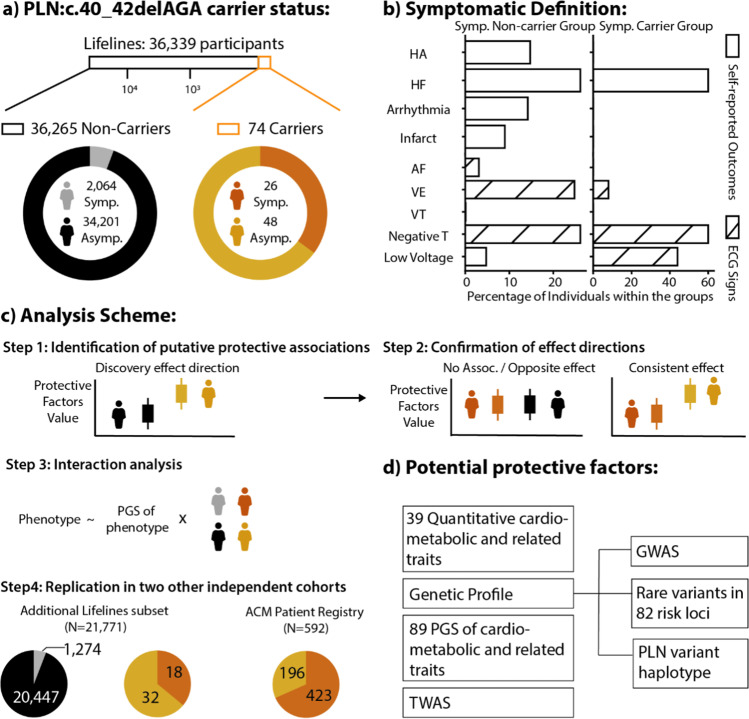
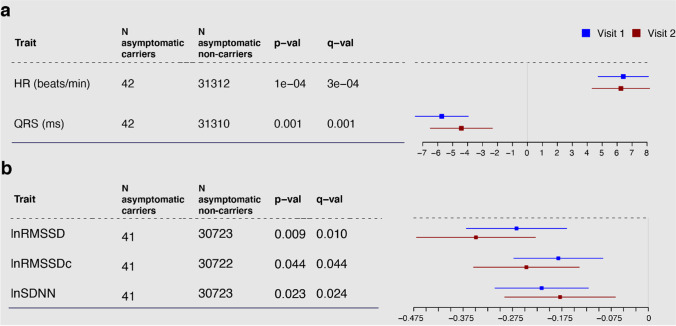
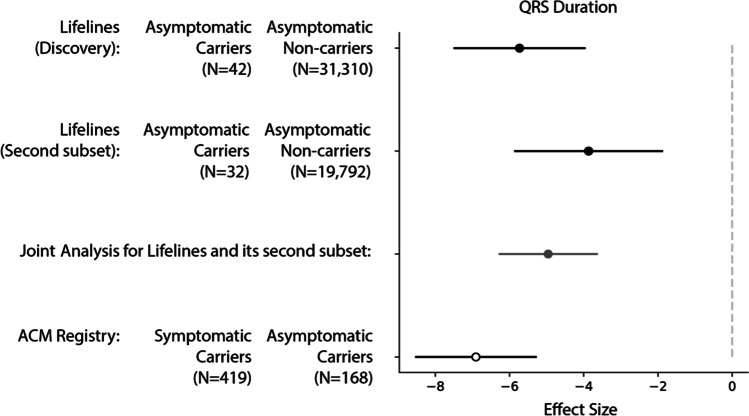
The c.40_42delAGA variant in the phospholamban gene (PLN) has been associated with dilated and arrhythmogenic cardiomyopathy, with up to 70% of carriers experiencing a major cardiac event by age 70. However, there are carriers who remain asymptomatic at older ages. To understand the mechanisms behind this incomplete penetrance, we evaluated potential phenotypic and genetic modifiers in 74 PLN:c.40_42delAGA carriers identified in 36,339 participants of the Lifelines population cohort. Asymptomatic carriers (N = 48) showed shorter QRS duration (- 5.73 ms, q value = 0.001) compared to asymptomatic non-carriers, an effect we could replicate in two different independent cohorts. Furthermore, symptomatic carriers showed a higher correlation (rPearson = 0.17) between polygenic predisposition to higher QRS (PGSQRS) and QRS (p value = 1.98 × 10-8), suggesting that the effect of the genetic variation on cardiac rhythm might be increased in symptomatic carriers. Our results allow for improved clinical interpretation for asymptomatic carriers, while our approach could guide future studies on genetic diseases with incomplete penetrance.
Keywords: Cardiomyopathy; Genome-wide association study; Incomplete penetrance; Modifiers of Mendelian disorders; Polygenic score.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Elliott P, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270–276. - PubMed
-
- McKenna WJ, Judge DP. Epidemiology of the inherited cardiomyopathies. Nat Rev Cardiol. 2021;18:22–36. - PubMed
-
- MacLennan DH, Kranias EG. Phospholamban: a crucial regulator of cardiac contractility. Nat Rev Mol Cell Biol. 2003;4:566–577. - PubMed
URLs
-
- Lifelines catalog. https://www.laifelines.nl/researcher/how-to-apply/catalogue.
-
- ACM/PLN Registry. https://www.acmregistry.nl/.
-
- FInnGen thermoFisher Axiom custom Array. https://www.finngen.fi/en/researchers/genotyping.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
