

Efficacy of Virtual Care for Depressive Disorders: Systematic Review and Meta-analysis
- PMID: 36622747
- PMCID: PMC9871881
- DOI: 10.2196/38955
Efficacy of Virtual Care for Depressive Disorders: Systematic Review and Meta-analysis
Abstract
Background: The COVID-19 pandemic has created an epidemic of distress-related mental disorders such as depression, while simultaneously necessitating a shift to virtual domains of mental health care; yet, the evidence to support the use of virtual interventions is unclear.
Objective: The purpose of this study was to evaluate the efficacy of virtual interventions for depressive disorders by addressing three key questions: (1) Does virtual intervention provide better outcomes than no treatment or other control conditions (ie, waitlist, treatment as usual [TAU], or attention control)? (2) Does in-person intervention provide better outcomes than virtual intervention? (3) Does one type of virtual intervention provide better outcomes than another?
Methods: We searched the PubMed, EMBASE, and PsycINFO databases for trials published from January 1, 2010, to October 30, 2021. We included randomized controlled trials of adults with depressive disorders that tested a virtual intervention and used a validated depression measure. Primary outcomes were defined as remission (ie, no longer meeting the clinical cutoff for depression), response (ie, a clinically significant reduction in depressive symptoms), and depression severity at posttreatment. Two researchers independently selected studies and extracted data using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Risk of bias was evaluated based on Agency for Healthcare and Research Quality guidelines. We calculated odds ratios (ORs) for binary outcomes and standardized mean differences (SMDs) for continuous outcomes.
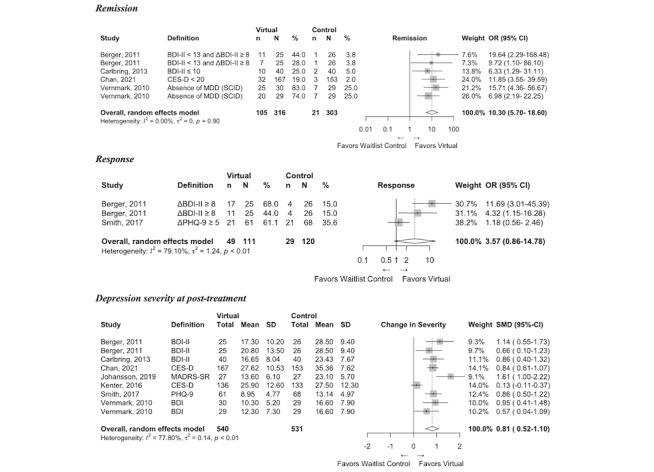
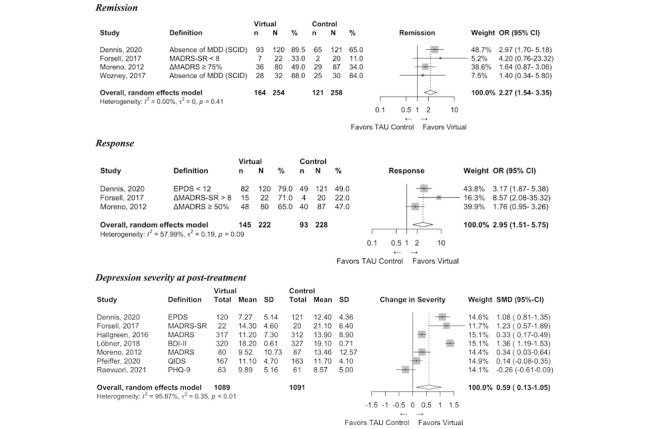
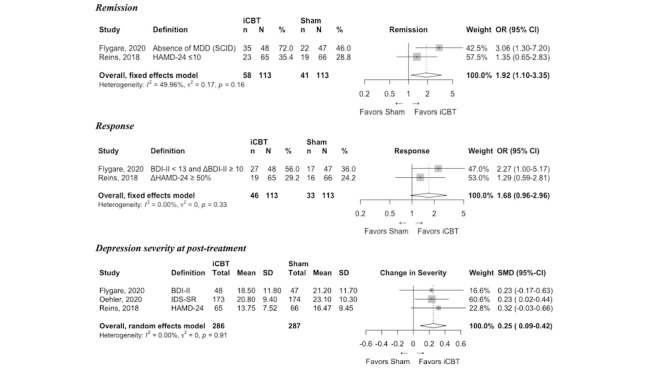
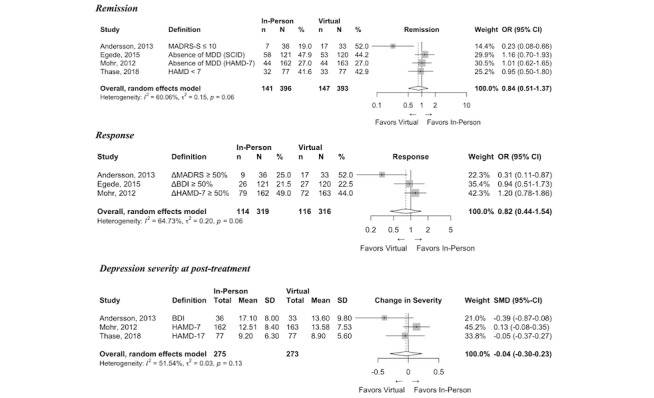
Results: We identified 3797 references, 24 of which were eligible. Compared with waitlist, virtual intervention had higher odds of remission (OR 10.30, 95% CI 5.70-18.60; N=619 patients) and lower posttreatment symptom severity (SMD 0.81, 95% CI 0.52-1.10; N=1071). Compared with TAU and virtual attention control conditions, virtual intervention had higher odds of remission (OR 2.27, 95% CI 1.10-3.35; N=512) and lower posttreatment symptom severity (SMD 0.25, 95% CI 0.09-0.42; N=573). In-person intervention outcomes were not significantly different from virtual intervention outcomes (eg, remission OR 0.84, CI 0.51-1.37; N=789). No eligible studies directly compared one active virtual intervention to another.
Conclusions: Virtual interventions were efficacious compared with control conditions, including waitlist control, TAU, and attention control. Although the number of studies was relatively small, the strength of evidence was moderate that in-person interventions did not yield significantly better outcomes than virtual interventions for depressive disorders.
Keywords: depression; depressive disorder; digital health; digital intervention; digital mental health; eHealth; efficacy; health intervention; health outcome; mental health; meta-analysis; review; therapy; treatment; virtual; virtual care; virtual intervention.
©Crystal Edler Schiller, Julianna Prim, Anna E Bauer, Linda Lux, Laura Claire Lundegard, Michelle Kang, Samantha Hellberg, Katherine Thompson, Theresa Webber, Adonay Teklezghi, Noah Pettee, Katherine Gaffney, Gabrielle Hodgins, Fariha Rahman, J Nikki Steinsiek, Anita Modi, Bradley N Gaynes. Originally published in JMIR Mental Health (https://mental.jmir.org), 09.01.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Hasin DS, Sarvet AL, Meyers JL, Saha TD, Ruan WJ, Stohl M, Grant BF. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry. 2018 Apr 01;75(4):336–346. doi: 10.1001/jamapsychiatry.2017.4602. https://europepmc.org/abstract/MED/29450462 2671413 - DOI - PMC - PubMed
-
- Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw Open. 2020 Sep 01;3(9):e2019686. doi: 10.1001/jamanetworkopen.2020.19686. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jam... 2770146 - DOI - DOI - PMC - PubMed
-
- Xiong J, Lipsitz O, Nasri F, Lui LM, Gill H, Phan L, Chen-Li D, Iacobucci M, Ho R, Majeed A, McIntyre RS. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020 Dec 01;277:55–64. doi: 10.1016/j.jad.2020.08.001. https://europepmc.org/abstract/MED/32799105 S0165-0327(20)32589-1 - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
