

Computer-aided diagnosis for optical diagnosis of diminutive colorectal polyps including sessile serrated lesions: a real-time comparison with screening endoscopists
- PMID: 36623839
- PMCID: PMC10374350
- DOI: 10.1055/a-2009-3990
Computer-aided diagnosis for optical diagnosis of diminutive colorectal polyps including sessile serrated lesions: a real-time comparison with screening endoscopists
Abstract
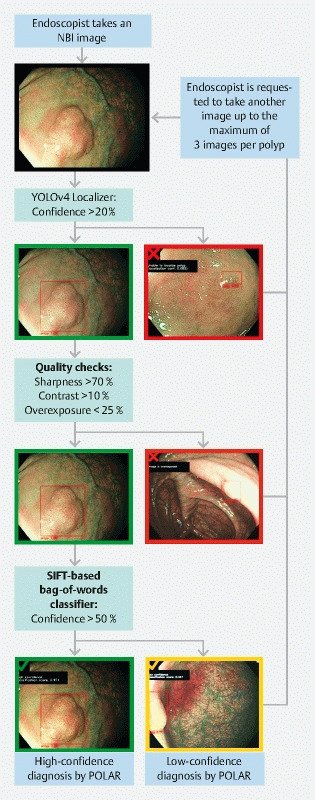
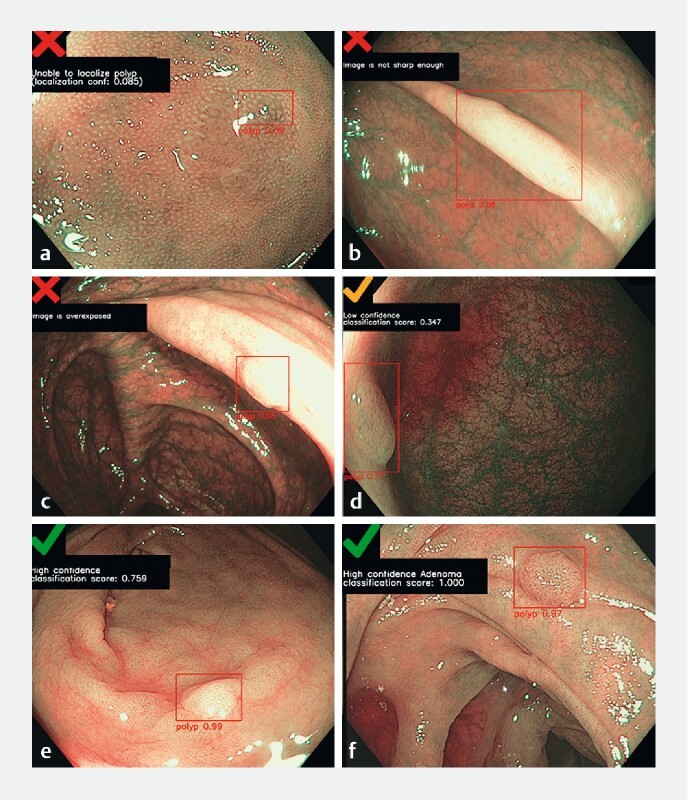
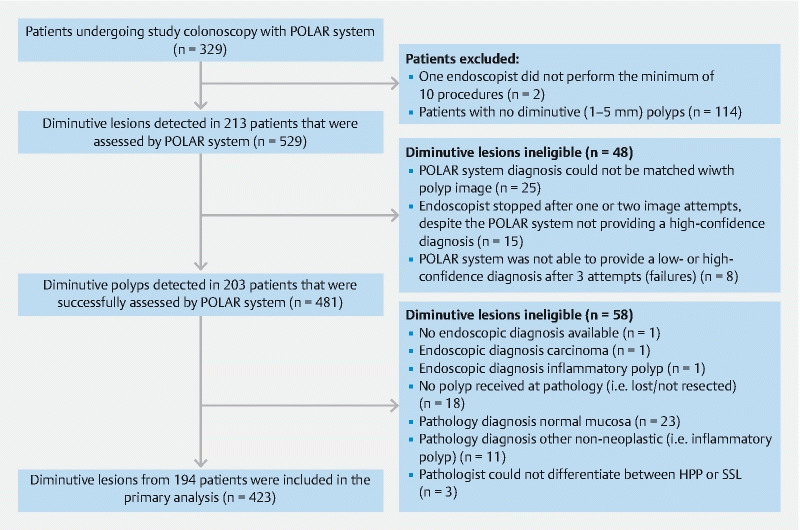
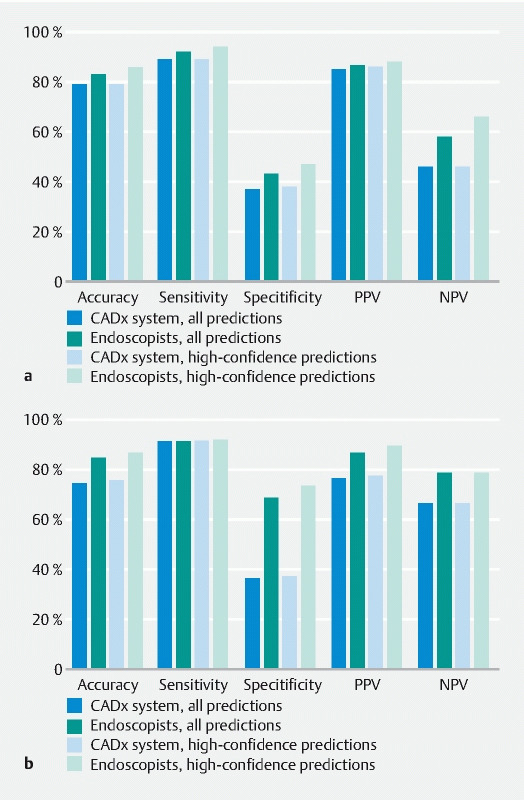
BACKGROUND : We aimed to compare the accuracy of the optical diagnosis of diminutive colorectal polyps, including sessile serrated lesions (SSLs), between a computer-aided diagnosis (CADx) system and endoscopists during real-time colonoscopy. METHODS : We developed the POLyp Artificial Recognition (POLAR) system, which was capable of performing real-time characterization of diminutive colorectal polyps. For pretraining, the Microsoft-COCO dataset with over 300 000 nonpolyp object images was used. For training, eight hospitals prospectively collected 2637 annotated images from 1339 polyps (i. e. publicly available online POLAR database). For clinical validation, POLAR was tested during colonoscopy in patients with a positive fecal immunochemical test (FIT), and compared with the performance of 20 endoscopists from eight hospitals. Endoscopists were blinded to the POLAR output. Primary outcome was the comparison of accuracy of the optical diagnosis of diminutive colorectal polyps between POLAR and endoscopists (neoplastic [adenomas and SSLs] versus non-neoplastic [hyperplastic polyps]). Histopathology served as the reference standard. RESULTS : During clinical validation, 423 diminutive polyps detected in 194 FIT-positive individuals were included for analysis (300 adenomas, 41 SSLs, 82 hyperplastic polyps). POLAR distinguished neoplastic from non-neoplastic lesions with 79 % accuracy, 89 % sensitivity, and 38 % specificity. The endoscopists achieved 83 % accuracy, 92 % sensitivity, and 44 % specificity. The optical diagnosis accuracy between POLAR and endoscopists was not significantly different (P = 0.10). The proportion of polyps in which POLAR was able to provide an optical diagnosis was 98 % (i. e. success rate). CONCLUSIONS : We developed a CADx system that differentiated neoplastic from non-neoplastic diminutive polyps during endoscopy, with an accuracy comparable to that of screening endoscopists and near-perfect success rate.
Trial registration: ClinicalTrials.gov NCT03822390.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
E. Dekker has received a research grant from Fujifilm, a consulting fee for medical advice from Olympus, Fujifilm, GI Supply, PAION, Ambu, and CPP-FAP, and speaker fees from Olympus, Roche, GI Supply, Norgine, Fujifilm, and IPSEN. P. Fockens has received research support from Boston Scientific, and a consulting fee from Olympus and Cook Endoscopy. B.B.S.L. Houwen, Y. Hazewinkel, I. Giotis, J.L.A. Vleugels, N.S. Mostafavi, and P. van Putten declare that they have no conflict of interest.
Figures
References
-
- Hewett D G, Kaltenbach T, Sano Y et al. Validation of a simple classification system for endoscopic diagnosis of small colorectal polyps using narrow-band imaging. Gastroenterology. 2012;143:599–607. - PubMed
-
- Houwen B, Hassan C, Coupé V MH et al. Definition of competence standards for optical diagnosis of diminutive colorectal polyps: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement. Endoscopy. 2022;54:88–99. - PubMed
-
- Rex D K, Kahi C, O’Brien M et al. The American Society for Gastrointestinal Endoscopy PIVI (Preservation and Incorporation of Valuable Endoscopic Innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc. 2011;73:419–422. - PubMed
-
- Ahmad O F, Soares A S, Mazomenos E et al. Artificial intelligence and computer-aided diagnosis in colonoscopy: current evidence and future directions. Lancet Gastroenterol Hepatol. 2019;4:71–80. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- the European Regional Development Fund region Northern-Netherlands/UP-18-00565
- PPP Allowance made available by Health~Holland, Top Sector Life Sciences & Health, to the Dutch Digestive Disease Foundation to stimulate public-private partnerships/TKI 18-01
- The province of Friesland/NA
- UP-18-00565/the European Regional Development Fund region Northern-Netherlands
- TKI 18-01/PPP Allowance made available by Health~Holland, Top Sector Life Sciences & Health, to the Dutch Digestive Disease Foundation to stimulate public-private partnerships