

Rapid prediction of secondary neurologic decline after traumatic brain injury: a data analytic approach
- PMID: 36624110
- PMCID: PMC9829683
- DOI: 10.1038/s41598-022-26318-4
Rapid prediction of secondary neurologic decline after traumatic brain injury: a data analytic approach
Abstract
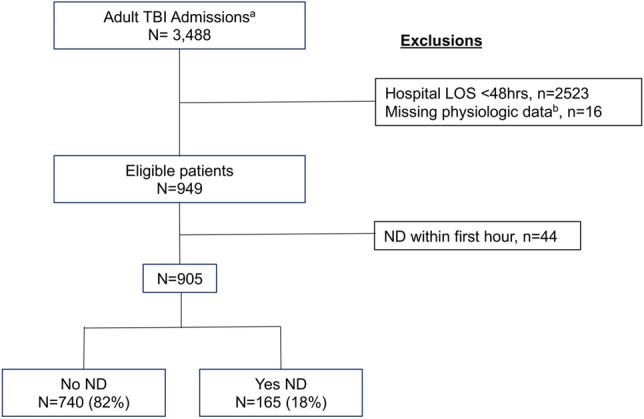
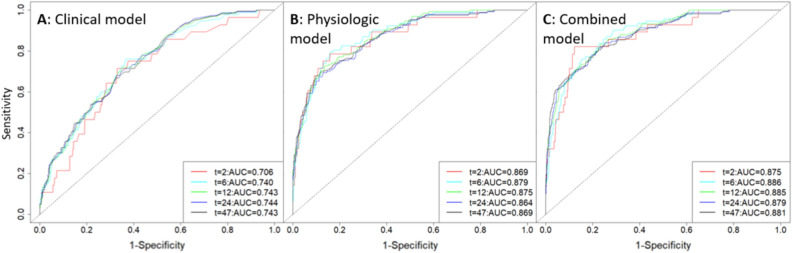
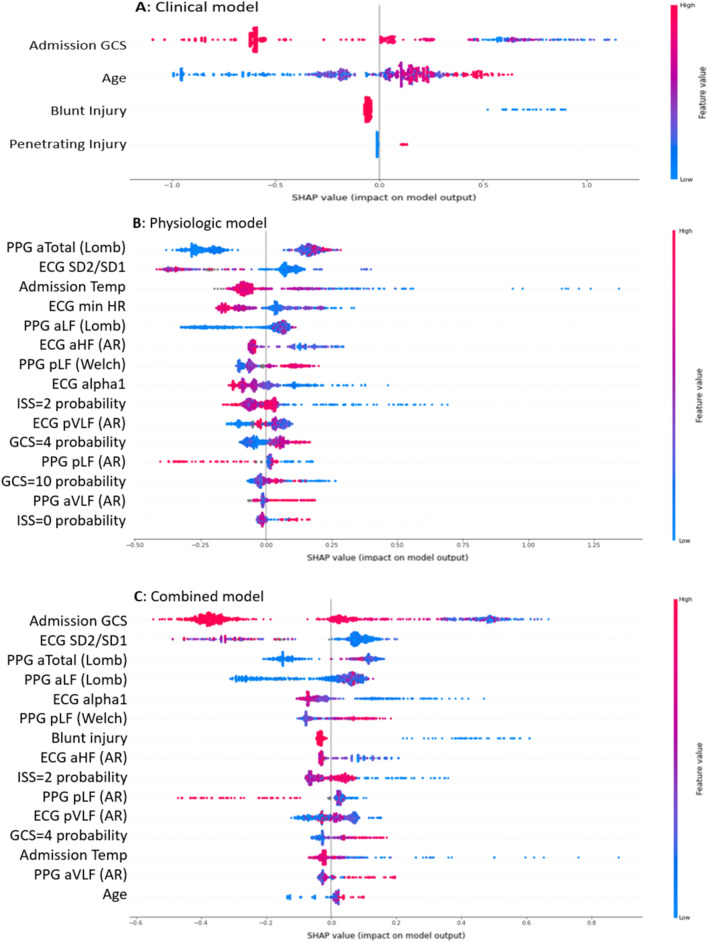
Secondary neurologic decline (ND) after traumatic brain injury (TBI) is independently associated with outcome, but robust predictors of ND are lacking. In this retrospective analysis of consecutive isolated TBI admissions to the R. Adams Cowley Shock Trauma Center between November 2015 and June 2018, we aimed to develop a triage decision support tool to quantify risk for early ND. Three machine learning models based on clinical, physiologic, or combined characteristics from the first hour of hospital resuscitation were created. Among 905 TBI cases, 165 (18%) experienced one or more ND events (130 clinical, 51 neurosurgical, and 54 radiographic) within 48 h of presentation. In the prediction of ND, the clinical plus physiologic data model performed similarly to the physiologic only model, with concordance indices of 0.85 (0.824-0.877) and 0.84 (0.812-0.868), respectively. Both outperformed the clinical only model, which had a concordance index of 0.72 (0.688-0.759). This preliminary work suggests that a data-driven approach utilizing physiologic and basic clinical data from the first hour of resuscitation after TBI has the potential to serve as a decision support tool for clinicians seeking to identify patients at high or low risk for ND.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Brain Trauma Foundation. https://www.braintrauma.org/faq.
-
- Otten EJ, Dorlac WC. Managing traumatic brain injury: Translating military guidelines to the wilderness. Wilderness Environ. Med. 2017;28:S117–S123. - PubMed
-
- Gurney JM, et al. The prehospital evaluation and care of moderate/severe TBI in the austere environment. Mil. Med. 2020;185:148–153. - PubMed
-
- Cowley R. Resuscitaion and stabilization of major multiple trauma patients in a trauma center environment. Clin. Med. 1976;83:16–22.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
