

Neural stem cell transplantation in patients with progressive multiple sclerosis: an open-label, phase 1 study
- PMID: 36624312
- PMCID: PMC9873560
- DOI: 10.1038/s41591-022-02097-3
Neural stem cell transplantation in patients with progressive multiple sclerosis: an open-label, phase 1 study
Abstract
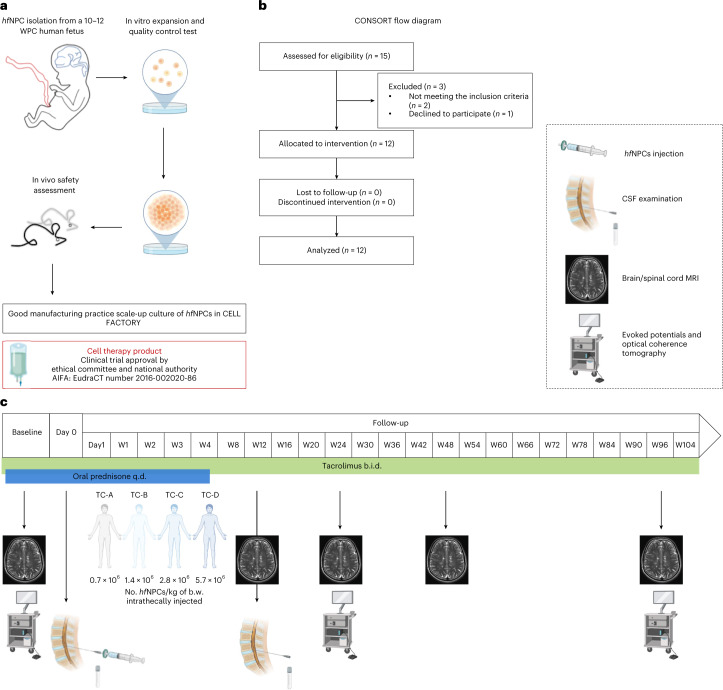
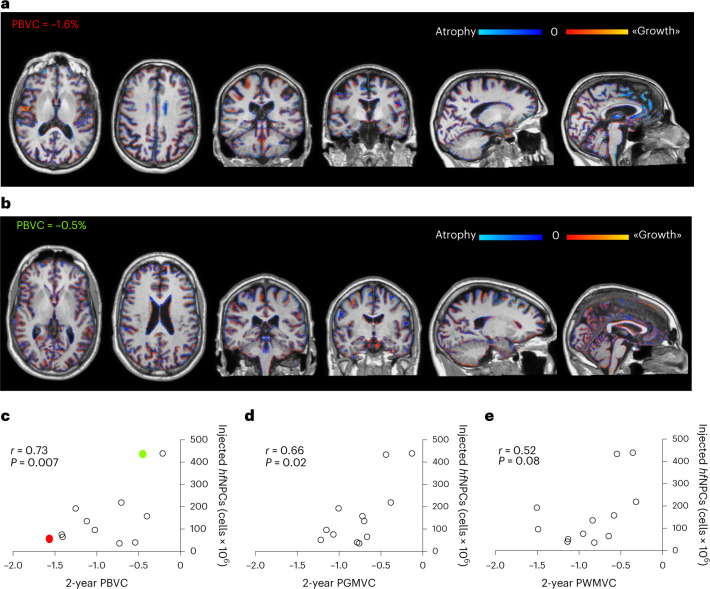
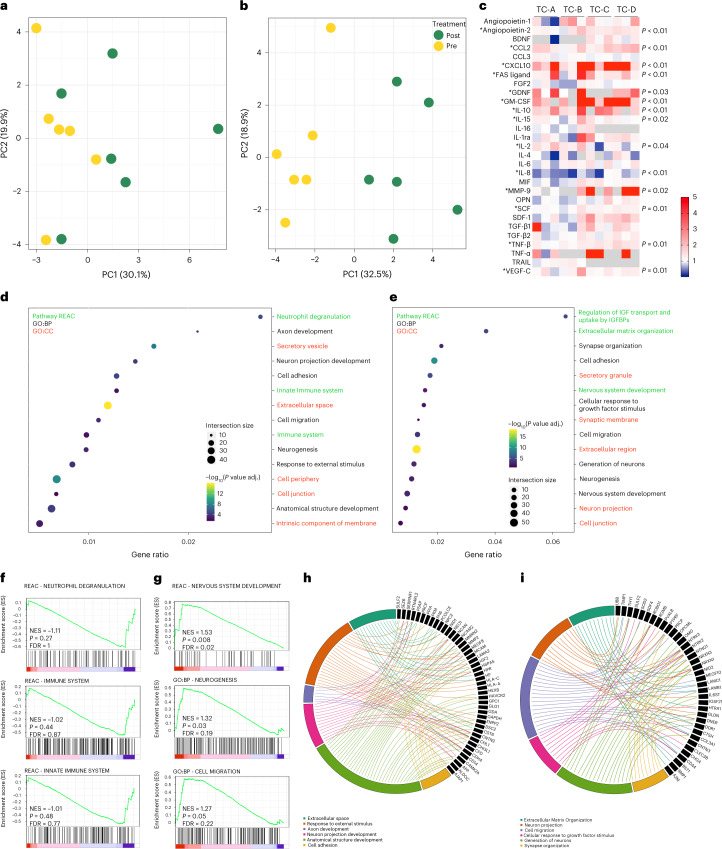
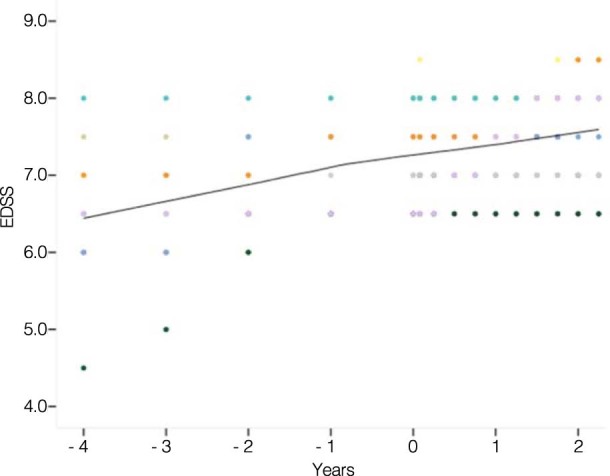
Innovative pro-regenerative treatment strategies for progressive multiple sclerosis (PMS), combining neuroprotection and immunomodulation, represent an unmet need. Neural precursor cells (NPCs) transplanted in animal models of multiple sclerosis have shown preclinical efficacy by promoting neuroprotection and remyelination by releasing molecules sustaining trophic support and neural plasticity. Here we present the results of STEMS, a prospective, therapeutic exploratory, non-randomized, open-label, single-dose-finding phase 1 clinical trial ( NCT03269071 , EudraCT 2016-002020-86), performed at San Raffaele Hospital in Milan, Italy, evaluating the feasibility, safety and tolerability of intrathecally transplanted human fetal NPCs (hfNPCs) in 12 patients with PMS (with evidence of disease progression, Expanded Disability Status Scale ≥6.5, age 18-55 years, disease duration 2-20 years, without any alternative approved therapy). The safety primary outcome was reached, with no severe adverse reactions related to hfNPCs at 2-year follow-up, clearly demonstrating that hfNPC therapy in PMS is feasible, safe and tolerable. Exploratory secondary analyses showed a lower rate of brain atrophy in patients receiving the highest dosage of hfNPCs and increased cerebrospinal fluid levels of anti-inflammatory and neuroprotective molecules. Although preliminary, these results support the rationale and value of future clinical studies with the highest dose of hfNPCs in a larger cohort of patients.
© 2023. The Author(s).
Conflict of interest statement
G.M. is the inventor of patent number EP1904073 (Europe) and US2008274089 (USA) filed on 12 July 2006. The other authors declare no competing interests.
Figures
Comment in
-
A neural stem-cell treatment for progressive multiple sclerosis.Nat Med. 2023 Jan;29(1):27-28. doi: 10.1038/s41591-022-02164-9. Nat Med. 2023. PMID: 36639562 No abstract available.
