

Comparison of hemodynamics during induction of general anesthesia with remimazolam and target-controlled propofol in middle-aged and elderly patients: a single-center, randomized, controlled trial
- PMID: 36624371
- PMCID: PMC9830695
- DOI: 10.1186/s12871-023-01974-9
Comparison of hemodynamics during induction of general anesthesia with remimazolam and target-controlled propofol in middle-aged and elderly patients: a single-center, randomized, controlled trial
Abstract
Background: Remimazolam confers a lower risk of hypotension than propofol. However, no studies have compared the efficacy of remimazolam and propofol administered using target-controlled infusion (TCI). This study aimed to investigate hemodynamic effects of remimazolam and target-controlled propofol in middle-aged and elderly patients during the induction of anesthesia.
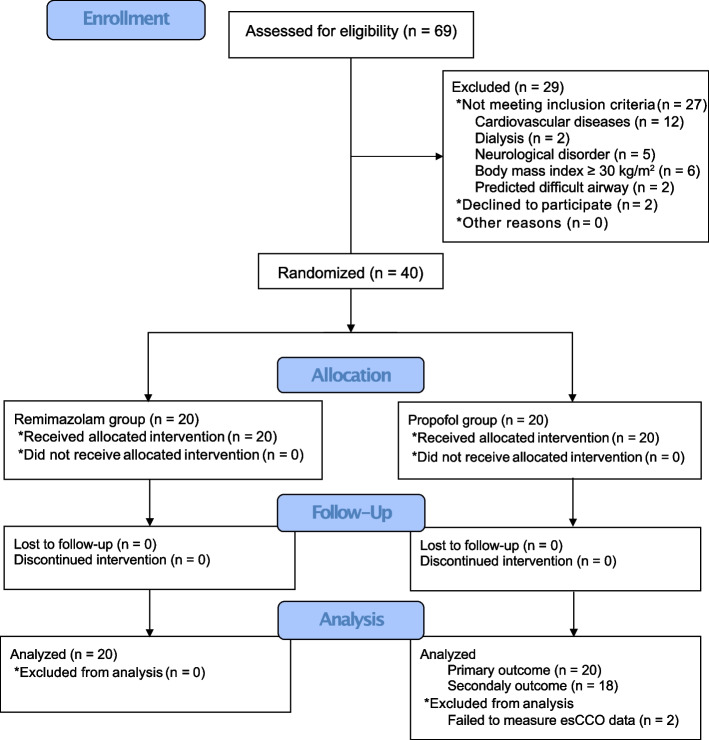
Methods: Forty adults aged 45-80 years with the American Society of Anesthesiologists Physical Status 1-2 were randomly assigned to remimazolam or propofol group (n = 20 each). Patients received either remimazolam (12 mg/kg/h) or propofol (3 μg/mL, TCI), along with remifentanil for inducing anesthesia. We recorded the blood pressure, heart rate (HR), and estimated continuous cardiac output (esCCO) using the pulse wave transit time. The primary outcome was the maximum change in mean arterial pressure (MAP) after induction. Secondary outcomes included changes in HR, cardiac output (CO), and stroke volume (SV).
Results: MAP decreased after induction of anesthesia in both groups, without significant differences between the groups (- 41.1 [16.4] mmHg and - 42.8 [10.8] mmHg in remimazolam and propofol groups, respectively; mean difference: 1.7 [95% confidence interval: - 8.2 to 4.9]; p = 0.613). Furthermore, HR, CO, and SV decreased after induction in both groups, without significant differences between the groups. Remimazolam group had significantly shorter time until loss of consciousness than propofol group (1.7 [0.7] min and 3.5 [1.7] min, respectively; p < 0.001). However, MAP, HR, CO, and SV were not significantly different between the groups despite adjusting time until loss of consciousness as a covariate. Seven (35%) and 11 (55%) patients in the remimazolam and propofol groups, respectively, experienced hypotension (MAP < 65 mmHg over 2.5 min), without significant differences between the groups (p = 0.341).
Conclusions: Hemodynamics were not significantly different between remimazolam and target-controlled propofol groups during induction of anesthesia. Thus, not only the choice but also the dose and usage of anesthetics are important for hemodynamic stability while inducing anesthesia. Clinicians should monitor hypotension while inducing anesthesia with remimazolam as well as propofol.
Trial registration: UMIN-CTR (UMIN000045612).
Keywords: Hemodynamics; Hypotension; Propofol; Remimazolam; Target-controlled infusion.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Sessler DI, Meyhoff CS, Zimmerman NM, Mao G, Leslie K, Vásquez SM, et al. Period-dependent associations between hypotension during and for four days after noncardiac surgery and a composite of myocardial infarction and death: a substudy of the POISE-2 Trial. Anesthesiology. 2018;128:317–327. doi: 10.1097/ALN.0000000000001985. - DOI - PubMed
-
- Walsh M, Devereaux PJ, Garg AX, Kurz A, Turan A, Rodseth RN, et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology. 2013;119:507–515. doi: 10.1097/ALN.0b013e3182a10e26. - DOI - PubMed
-
- Roshanov PS, Sheth T, Duceppe E, Tandon V, Bessissow A, Chan MTV, et al. Relationship between perioperative hypotension and perioperative cardiovascular events in patients with coronary artery disease undergoing major noncardiac surgery. Anesthesiology. 2019;130:756–766. doi: 10.1097/ALN.0000000000002654. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
