Expert consensus on the management of systemic sclerosis-associated interstitial lung disease
- PMID: 36624431
- PMCID: PMC9830797
- DOI: 10.1186/s12931-022-02292-3
Expert consensus on the management of systemic sclerosis-associated interstitial lung disease
Abstract
Background: Systemic sclerosis (SSc) is a rare, complex, connective tissue disorder. Interstitial lung disease (ILD) is common in SSc, occurring in 35-52% of patients and accounting for 20-40% of mortality. Evolution of therapeutic options has resulted in a lack of consensus on how to manage this condition. This Delphi study was initiated to develop consensus recommendations based on expert physician insights regarding screening, progression, treatment criteria, monitoring of response, and the role of recent therapeutic advances with antifibrotics and immunosuppressants in patients with SSc-ILD.
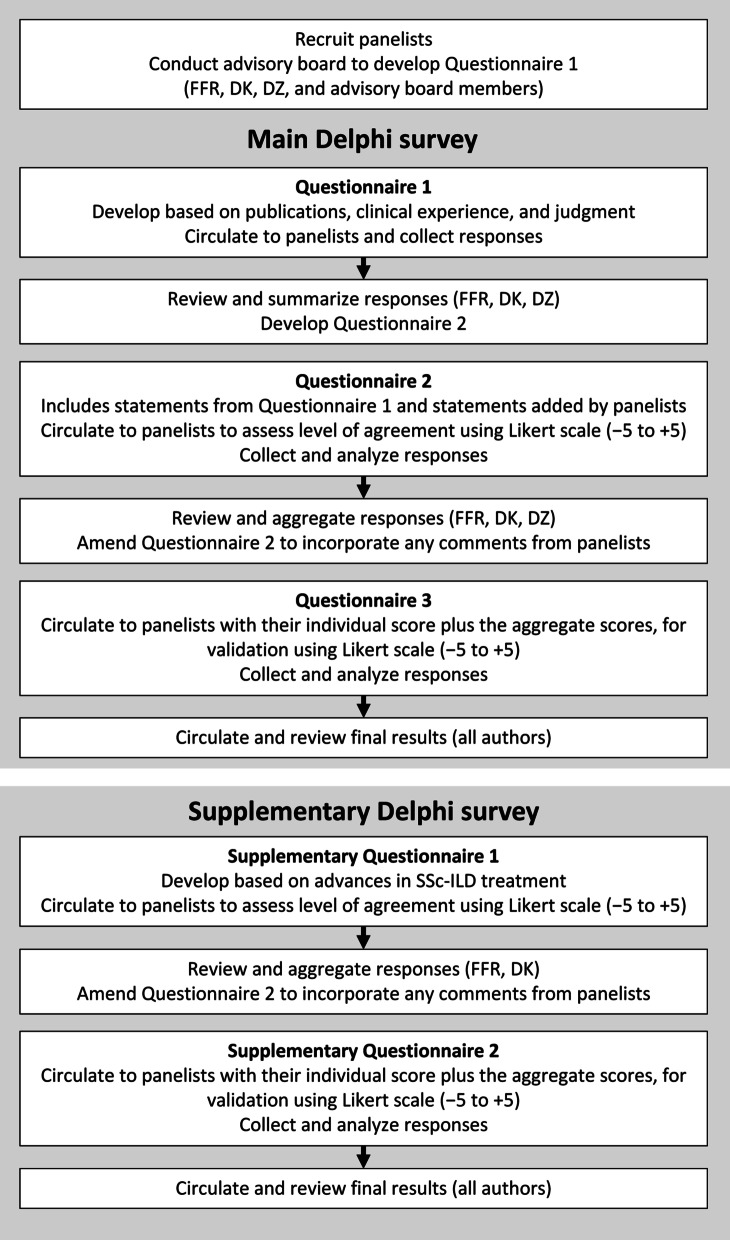
Methods: A modified Delphi process was completed by pulmonologists (n = 13) and rheumatologists (n = 12) with expertise in the management of patients with SSc-ILD. Panelists rated their agreement with each statement on a Likert scale from - 5 (complete disagreement) to + 5 (complete agreement). Consensus was predefined as a mean Likert scale score of ≤ - 2.5 or ≥ + 2.5 with a standard deviation not crossing zero.
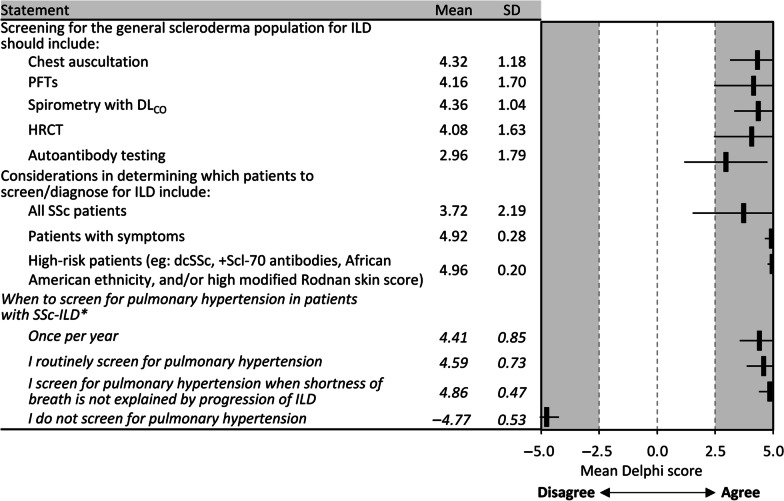
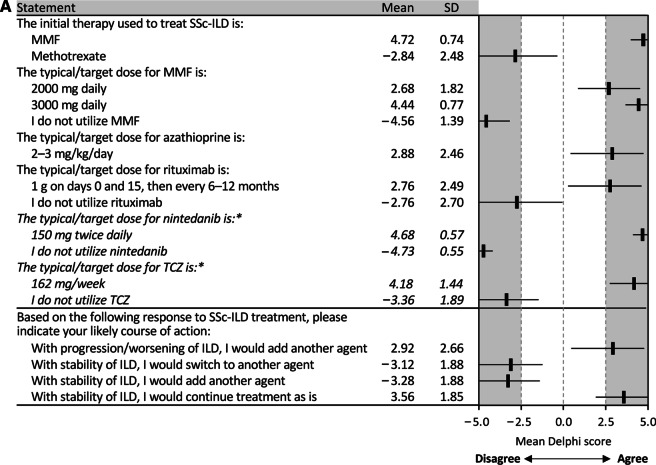
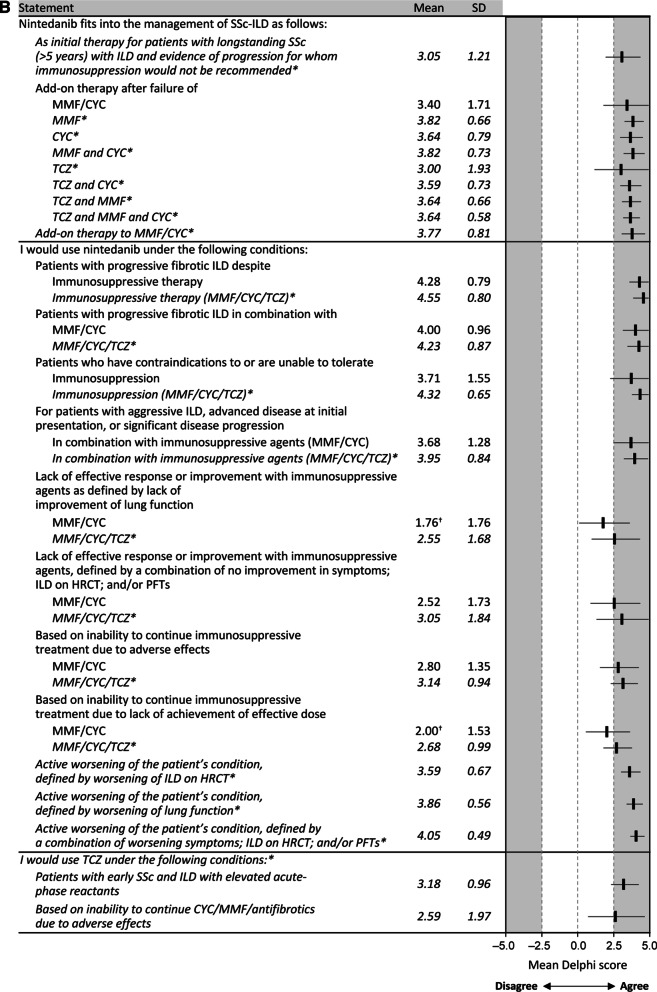
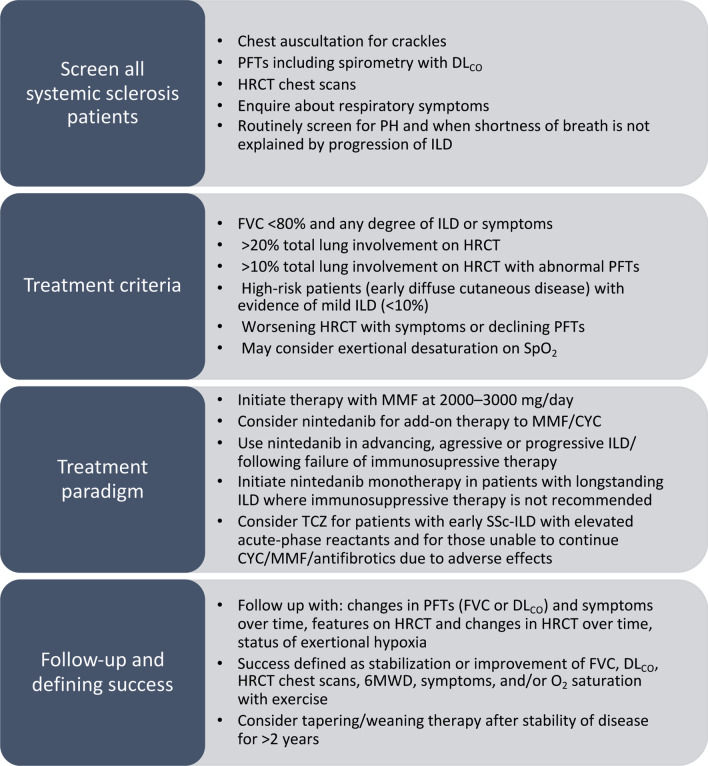
Results: Panelists recommended that all patients with SSc be screened for ILD by chest auscultation, spirometry with diffusing capacity of the lungs for carbon monoxide, high-resolution computed tomography (HRCT), and/or autoantibody testing. Treatment decisions were influenced by baseline and changes in pulmonary function tests, extent of ILD on HRCT, duration and degree of dyspnea, presence of pulmonary hypertension, and potential contribution of reflux. Treatment success was defined as stabilization or improvement of signs or symptoms of ILD and functional status. Mycophenolate mofetil was identified as the initial treatment of choice. Experts considered nintedanib a therapeutic option in patients with progressive fibrotic ILD despite immunosuppressive therapy or patients contraindicated/unable to tolerate immunotherapy. Concomitant use of nintedanib with MMF/cyclophosphamide can be considered in patients with advanced disease at initial presentation, aggressive ILD, or significant disease progression. Although limited consensus was achieved on the use of tocilizumab, the experts considered it a therapeutic option for patients with early SSc and ILD with elevated acute-phase reactants.
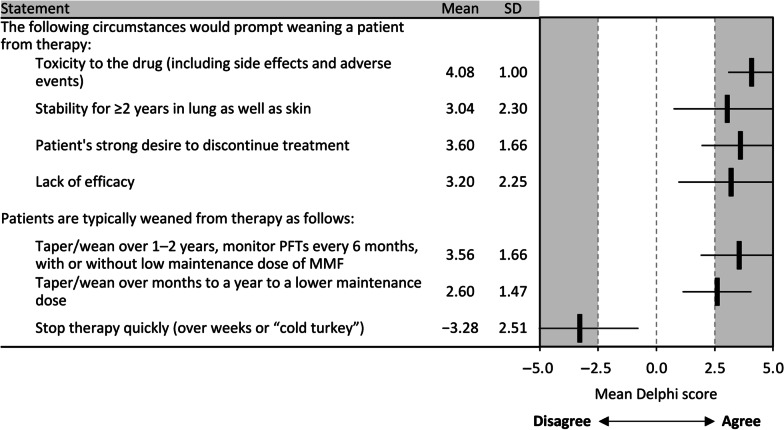
Conclusions: This modified Delphi study generated consensus recommendations for management of patients with SSc-ILD in a real-world setting. Findings from this study provide a management algorithm that will be helpful for treating patients with SSc-ILD and addresses a significant unmet need.
Keywords: Algorithms; Autoimmune diseases; Connective tissue diseases; Drug therapy; Pulmonary fibrosis.
© 2023. The Author(s).
Conflict of interest statement
FFR reports personal fees from Boehringer Ingelheim (BI) and Genentech. VMH reports personal fees from BI. RJK reports grants and personal fees from BI; personal fees from Galapagos, Genentech, Pliant, PureTech and United Therapeutics; and participation in clinical trials for Bellerophon, Respivant and Toray. MDM reports participation in clinical trials for Bayer, Corbus Pharmaceuticals, Eicos Sciences, Reata, Sanofi; and personal fees from Actelion Pharma, Astellas, BI, Galapagos, Medtelligence, and Mitsubishi Tanabe Pharma. IOR reports personal fees from BI and participation in a clinical trial for Genentech. RS reports grants and personal fees from Acceleron Pharma, Actelion, and United Therapeutics; grants from Bellerophon; and personal fees from Third Pole. VDS reports participation in Steering Committees for studies sponsored by CSL Behring and Eicos Sciences; grants and personal fees from BI, Corbus Pharmaceuticals, CSL Behring, and Eicos Sciences; and participation in clinical trials for BI, CSL Behring, Corbus Pharmaceuticals, and Eicos Sciences. MES reports grants, personal fees and non-financial support from BI; grants from Galapagos, the National Institute of Health, and the Pulmonary Fibrosis Foundation; and personal fees from FibroGen. EJB reports grants and personal fees from BI and Eicos Sciences and grants from Corbus Pharmaceuticals and Pfizer. FVC reports personal fees from BI. LC reports participation in Steering Committees for studies sponsored by Eicos Sciences; membership of the Data and Safety Monitoring Board for studies supported by Reata; grants and personal fees from BI; and personal fees from Eicos Sciences, Genentech and Mitsubishi Tanabe Pharma. RTD reports personal fees from BI, Eicos Sciences and Formation Biologics. KRF reports grants and personal fees from BI and Roche/Genentech and personal fees from Bellerophon, Blade Therapeutics, DevPro, Horizon Pharmaceuticals, PureHealth, Respivant, Shionogi, and United Therapeutics. FJM reports participation in Steering Committees for studies sponsored by Afferent/Merck, AstraZeneca, Bayer, Biogen, Chiesi, Gilead, GlaxoSmithKline, Nitto, Patara/Respivant, ProMedior/Roche, Prometic, and Veracyte; being a member of the Data and Safety Monitoring Board for studies supported by BI, Biogen, Genentech, and GlaxoSmithKline; personal fees and non-financial support from AstraZeneca, BI, the Canadian Respiratory Network, Chiesi, CSL Behring, Genentech, GlaxoSmithKline, Miller Communications, the National Society for Continuing Education, PeerView Communications, Physicians Education Resource, Sanofi/Regeneron, Sunovion, and Teva; non-financial support from ProterrixBio and Zambon; personal fees from the Academy for Continuing Healthcare Learning, American Thoracic Society, Bayer, Bridge Biotherapeutics, CME Outfitters, Dartmouth University, DevPro, Gala, Integritas, IQVIA, MD Magazine, Methodist Hospital Brooklyn, New York University, Projects in Knowledge, Rockpointe, United Therapeutics, UpToDate, Vindico, and WebMD/MedScape; grants from the National Institute for Health, ProMedior/Roche and Rare Disease Healthcare Communications; and non-financial interactions with AbbVie and twoXAR. NP, affiliated with Columbia University Irving Medical Center during the Delphi study, is now an employee of BI. OAS reports consulting fees from United Therapeutics, Altavant and Acceleron Pharma; and is on the speaker bureaus for United Therapeutics, Janssen Pharmaceuticals and Bayer. ERV reports grants from Corbus Pharmaceuticals, Forbius, and Kadmon, and personal fees from BI. DK reports grants and personal fees from Bayer, Bristol-Myers Squibb and Genentech/Roche; personal fees from Acceleron, Actelion, Blade Therapeutics, Eicos Sciences, Galapagos, GlaxoSmithKline, Mitsubishi Tanabe, Sanofi-Aventis/Genzyme, and UCB Pharma; and participation in clinical trials for Bayer, Bristol-Myers Squibb, GlaxoSmithKline, and Sanofi-Aventis/Genzyme. BDS, BK, LEM, NB, NG, and TM have nothing to disclose.
Figures