

ENDOTHELIAL GLYCOCALYX SHEDDING IN INTRA-ABDOMINAL SEPSIS: A FEASIBILITY STUDY
- PMID: 36625488
- PMCID: PMC11213624
- DOI: 10.1097/SHK.0000000000002079
ENDOTHELIAL GLYCOCALYX SHEDDING IN INTRA-ABDOMINAL SEPSIS: A FEASIBILITY STUDY
Abstract
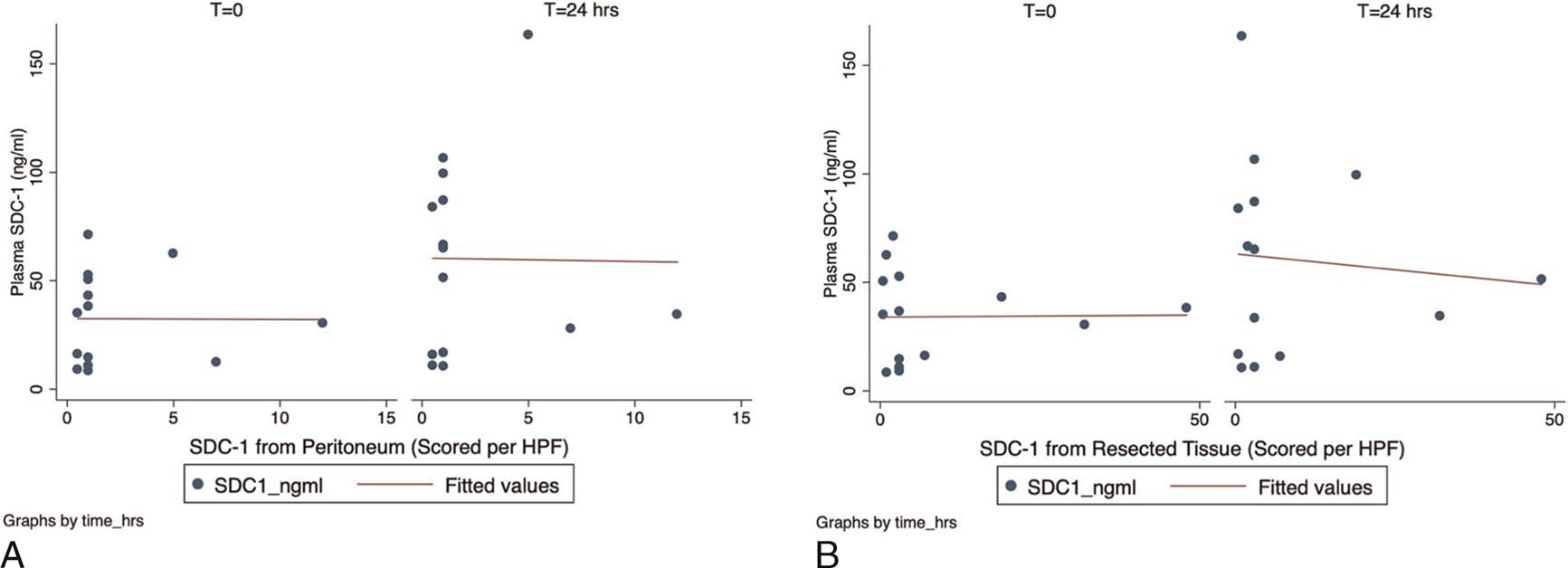
Background: The endothelial glycocalyx layer (EGL) is a complex meshwork of glycosaminoglycans and proteoglycans that protect the vascular endothelium. Cleavage or shedding of EGL-specific biomarkers, such as hyaluronic acid (HA) and syndecan-1 (SDC-1, CD138) in plasma, have been shown to be associated with poor clinical outcomes. However, it is unclear whether levels of circulating EGL biomarkers are representative of the EGL injury within the tissues. The objective of the present feasibility study was to describe a pathway for plasma and tissue procurement to quantify EGL components in a cohort of surgical patients with intra-abdominal sepsis. We sought to compare differences between tissue and plasma EGL biomarkers and to determine whether EGL shedding within the circulation and/or tissues correlated with clinical outcomes. Methods: This was a prospective, observational, single-center feasibility study of adult patients (N = 15) with intra-abdominal sepsis, conducted under an approved institutional review boards. Blood and resected tissue (pathologic specimen and unaffected peritoneum) samples were collected from consented subjects at the time of operation and 24-48 hours after surgery. Endothelial glycocalyx layer biomarkers (i.e., HA and SDC-1) were quantified in both tissue and plasma samples using a CD138 stain and ELISA kit, respectively. Pairwise comparisons were made between plasma and tissue levels. In addition, we tested the relationships between measured EGL biomarkers and clinical status and patient outcomes. Results: Fifteen patients with intra-abdominal sepsis were enrolled in the study. Elevations in EGL-specific circulating biomarkers (HA, SDC-1) were positively correlated with postoperative SOFA scores and weakly associated with resuscitative volumes at 24 hours. Syndecan-1 levels from resected pathologic tissue significantly correlated with SOFA scores at all time points ( R = 0.69 and P < 0.0001) and positively correlated with resuscitation volumes at 24 hours ( R = 0.41 and P = 0.15 for t = 24 hours). Tissue and circulating HA and SDC-1 positively correlated with SOFA >6. Conclusions: Elevations in both circulating and tissue EGL biomarkers were positively correlated with postoperative SOFA scores at 24 hours, with resected pathologic tissue EGL levels displaying significant correlations with SOFA scores at all time points. Tissue and circulating EGL biomarkers were positively correlated at higher SOFA scores (SOFA > 6) and could be used as indicators of resuscitative needs within 24 hours of surgery. The present study demonstrates the feasibility of tissue and plasma procurement in the operating room, although larger studies are needed to evaluate the predictive value of these EGL biomarkers for patients with intra-abdominal sepsis.
Copyright © 2023 by the Shock Society.
Figures




References
-
- Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49:E1063–E1143. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
