

Current and Emerging Knowledge in COVID-19
- PMID: 36625747
- PMCID: PMC9846833
- DOI: 10.1148/radiol.222462
Current and Emerging Knowledge in COVID-19
Abstract
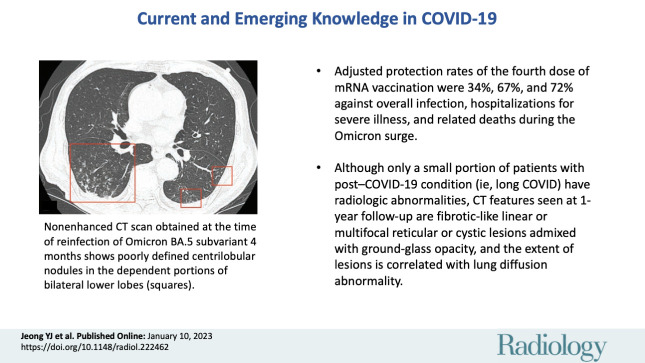
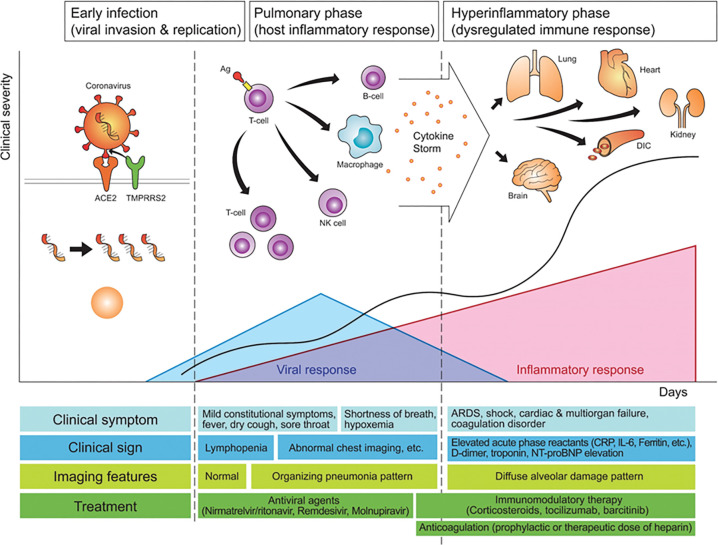
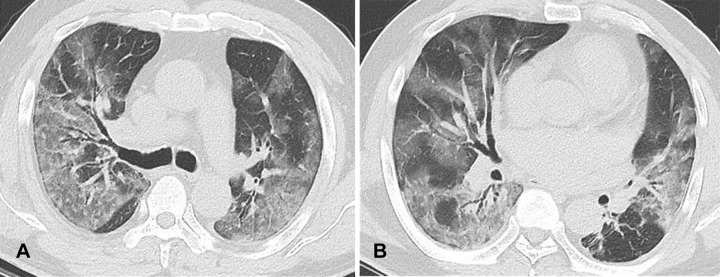
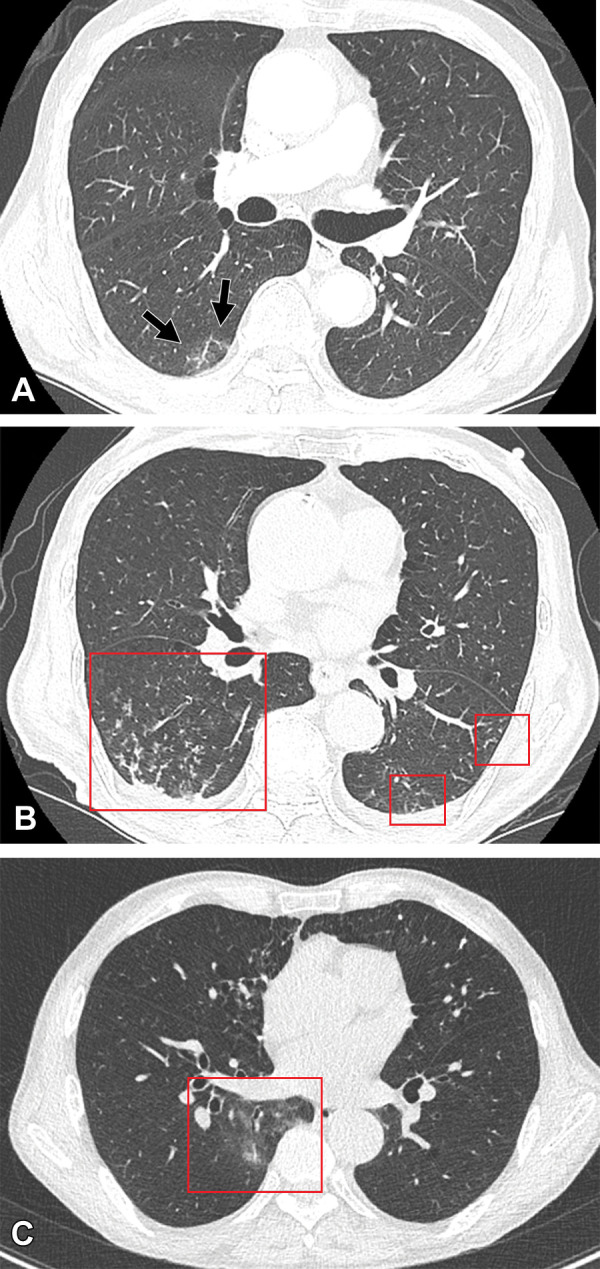
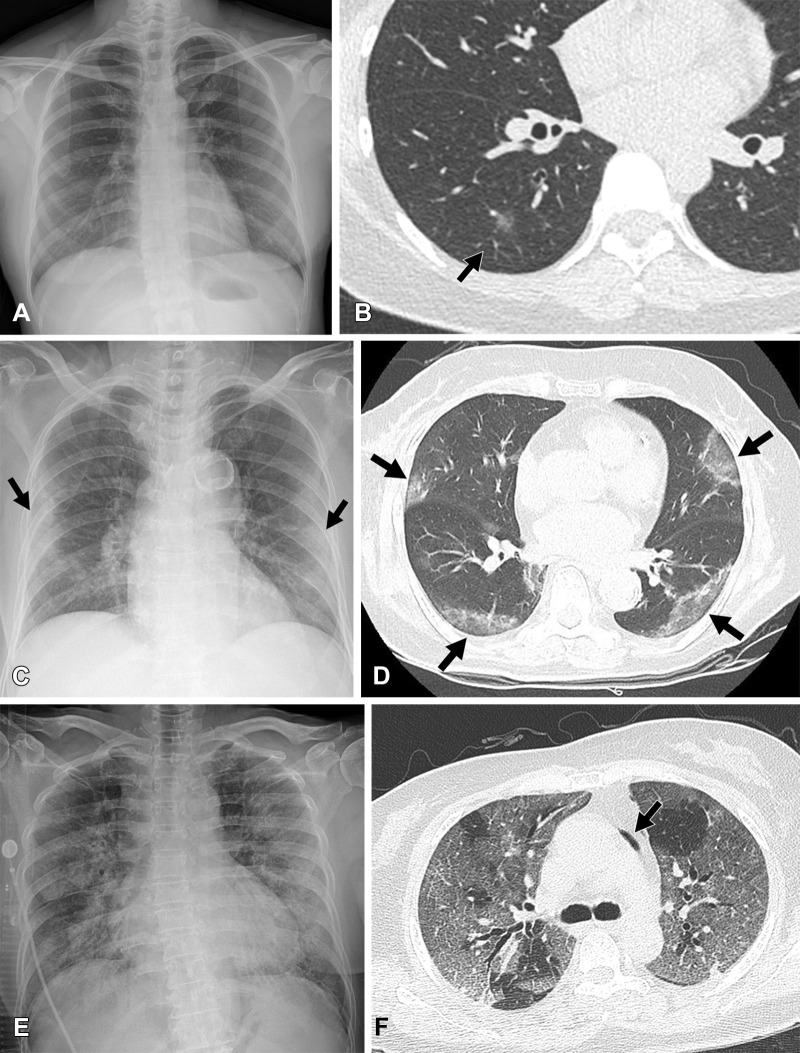
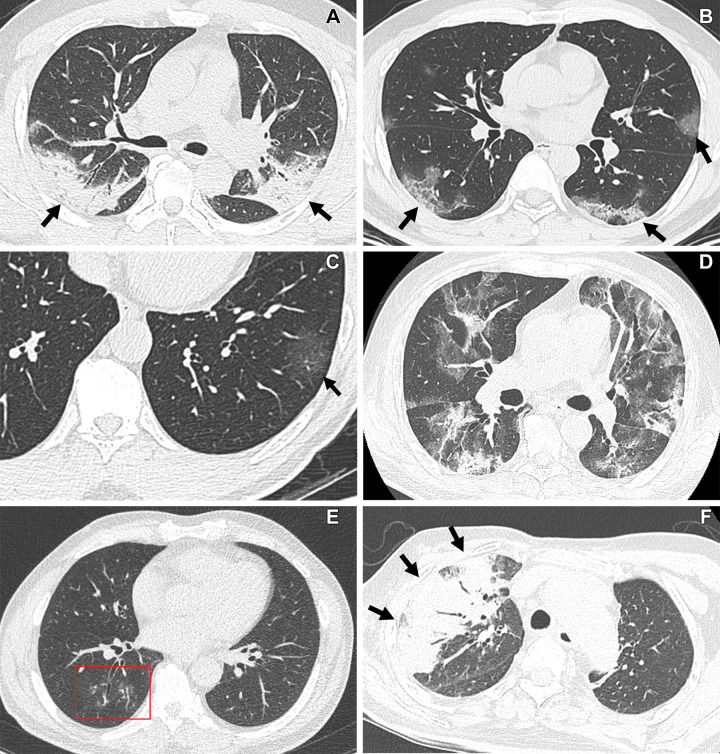
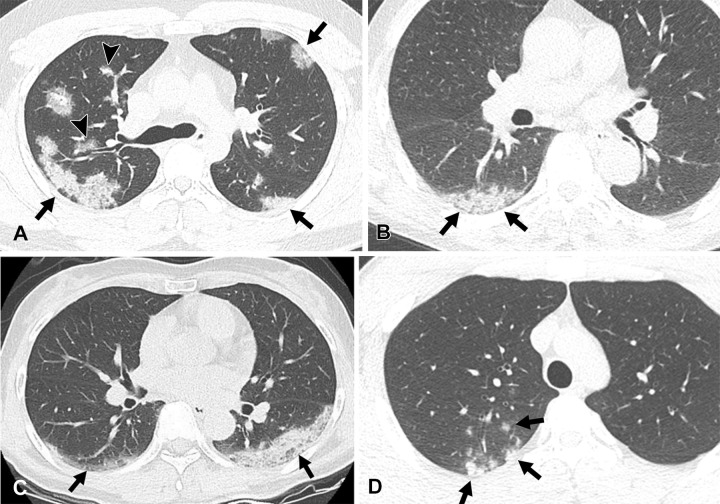
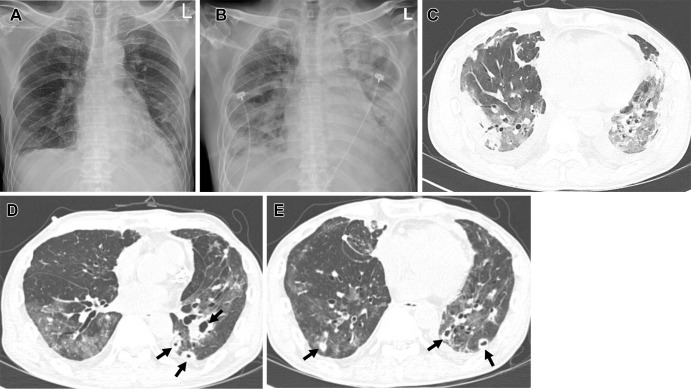
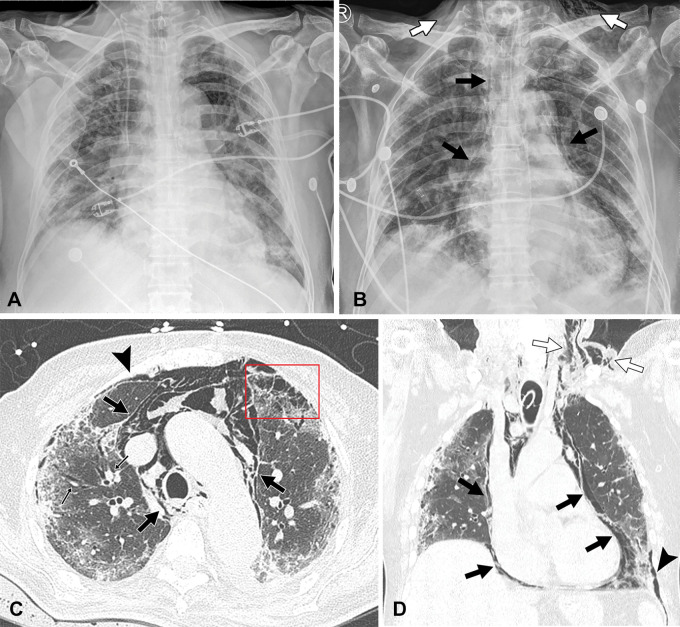
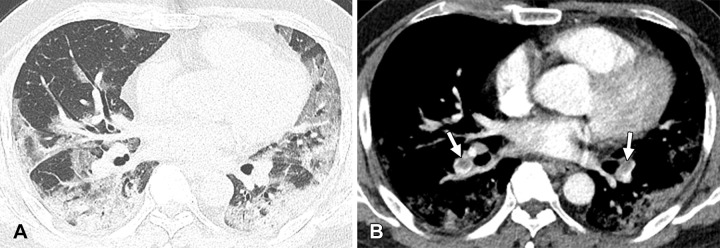
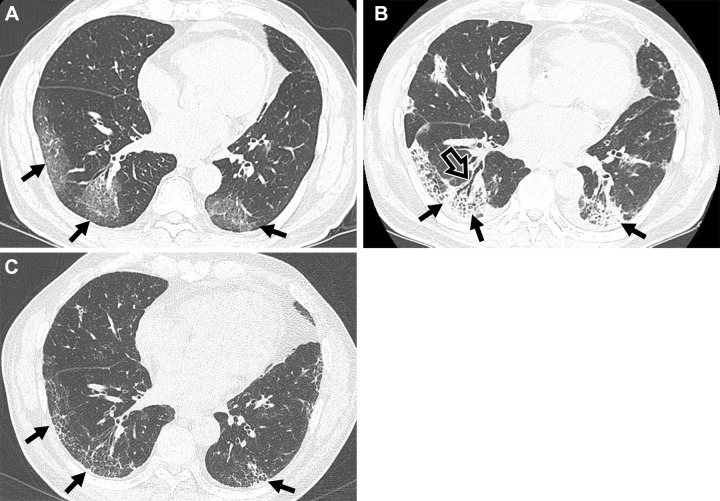
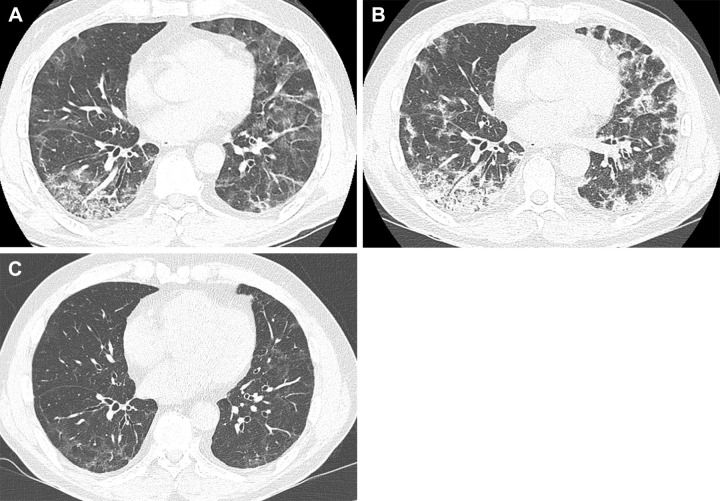
COVID-19 has emerged as a pandemic leading to a global public health crisis of unprecedented morbidity. A comprehensive insight into the imaging of COVID-19 has enabled early diagnosis, stratification of disease severity, and identification of potential sequelae. The evolution of COVID-19 can be divided into early infectious, pulmonary, and hyperinflammatory phases. Clinical features, imaging features, and management are different among the three phases. In the early stage, peripheral ground-glass opacities are predominant CT findings, and therapy directly targeting SARS-CoV-2 is effective. In the later stage, organizing pneumonia or diffuse alveolar damage pattern are predominant CT findings and anti-inflammatory therapies are more beneficial. The risk of severe disease or hospitalization is lower in breakthrough or Omicron variant infection compared with nonimmunized or Delta variant infections. The protection rates of the fourth dose of mRNA vaccination were 34% and 67% against overall infection and hospitalizations for severe illness, respectively. After acute COVID-19 pneumonia, most residual CT abnormalities gradually decreased in extent, but they may remain as linear or multifocal reticular or cystic lesions. Advanced insights into the pathophysiologic and imaging features of COVID-19 along with vaccine benefits have improved patient care, but emerging knowledge of post-COVID-19 condition, or long COVID, also presents radiology with new challenges.
© RSNA, 2023.
Conflict of interest statement
Figures
References
-
- WHO Coronavirus disease dashboard . World Health Organization . https://covid19.who.int/. Accessed November 11, 2022 .
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
