

The Precision in Psychiatry (PIP) study: Testing an internet-based methodology for accelerating research in treatment prediction and personalisation
- PMID: 36627607
- PMCID: PMC9832676
- DOI: 10.1186/s12888-022-04462-5
The Precision in Psychiatry (PIP) study: Testing an internet-based methodology for accelerating research in treatment prediction and personalisation
Abstract
Background: Evidence-based treatments for depression exist but not all patients benefit from them. Efforts to develop predictive models that can assist clinicians in allocating treatments are ongoing, but there are major issues with acquiring the volume and breadth of data needed to train these models. We examined the feasibility, tolerability, patient characteristics, and data quality of a novel protocol for internet-based treatment research in psychiatry that may help advance this field.
Methods: A fully internet-based protocol was used to gather repeated observational data from patient cohorts receiving internet-based cognitive behavioural therapy (iCBT) (N = 600) or antidepressant medication treatment (N = 110). At baseline, participants provided > 600 data points of self-report data, spanning socio-demographics, lifestyle, physical health, clinical and other psychological variables and completed 4 cognitive tests. They were followed weekly and completed another detailed clinical and cognitive assessment at week 4. In this paper, we describe our study design, the demographic and clinical characteristics of participants, their treatment adherence, study retention and compliance, the quality of the data gathered, and qualitative feedback from patients on study design and implementation.
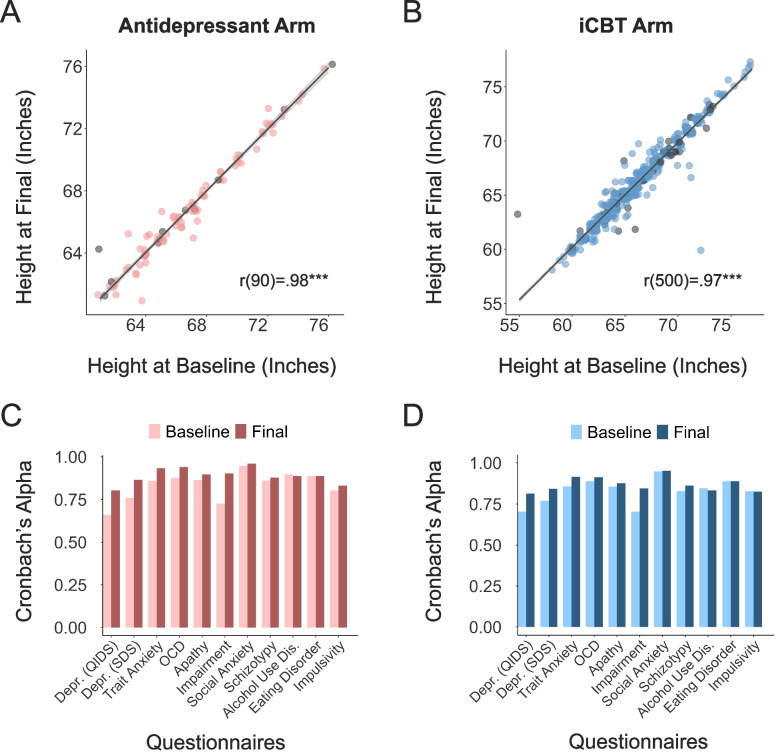
Results: Participant retention was 92% at week 3 and 84% for the final assessment. The relatively short study duration of 4 weeks was sufficient to reveal early treatment effects; there were significant reductions in 11 transdiagnostic psychiatric symptoms assessed, with the largest improvement seen for depression. Most participants (66%) reported being distracted at some point during the study, 11% failed 1 or more attention checks and 3% consumed an intoxicating substance. Data quality was nonetheless high, with near perfect 4-week test retest reliability for self-reported height (ICC = 0.97).
Conclusions: An internet-based methodology can be used efficiently to gather large amounts of detailed patient data during iCBT and antidepressant treatment. Recruitment was rapid, retention was relatively high and data quality was good. This paper provides a template methodology for future internet-based treatment studies, showing that such an approach facilitates data collection at a scale required for machine learning and other data-intensive methods that hope to deliver algorithmic tools that can aid clinical decision-making in psychiatry.
Keywords: Antidepressant; Big data; Internet-based methodology; Internet-delivered cognitive behavioural therapy; Mental health treatments; Treatment outcomes; Treatment prediction; Treatment response.
© 2023. The Author(s).
Conflict of interest statement
The PhD studentship of CTL is co-funded by SilverCloud Health and the Irish Research Council. JP, DR, and SH are current employees of SilverCloud Health. AKH, KL, NC, LS, VOK, KES, and CMG have no competing interests.
Figures






References
-
- Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, Norquist G, Howland RH, Lebowitz B, McGrath PJ, Shores-Wilson K. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR* D: implications for clinical practice. Am J Psychiatry. 2006;163(1):28–40. doi: 10.1176/appi.ajp.163.1.28. - DOI - PubMed
-
- Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, Niederehe G, Thase ME, Lavori PW, Lebowitz BD, McGrath PJ. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR* D report. Am J Psychiatry. 2006;163(11):1905–1917. doi: 10.1176/ajp.2006.163.11.1905. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
