

Cone beam computed tomography in the assessment of TMJ deformity in children with JIA: repeatability of a novel scoring system
- PMID: 36627622
- PMCID: PMC9830735
- DOI: 10.1186/s12903-022-02701-5
Cone beam computed tomography in the assessment of TMJ deformity in children with JIA: repeatability of a novel scoring system
Abstract
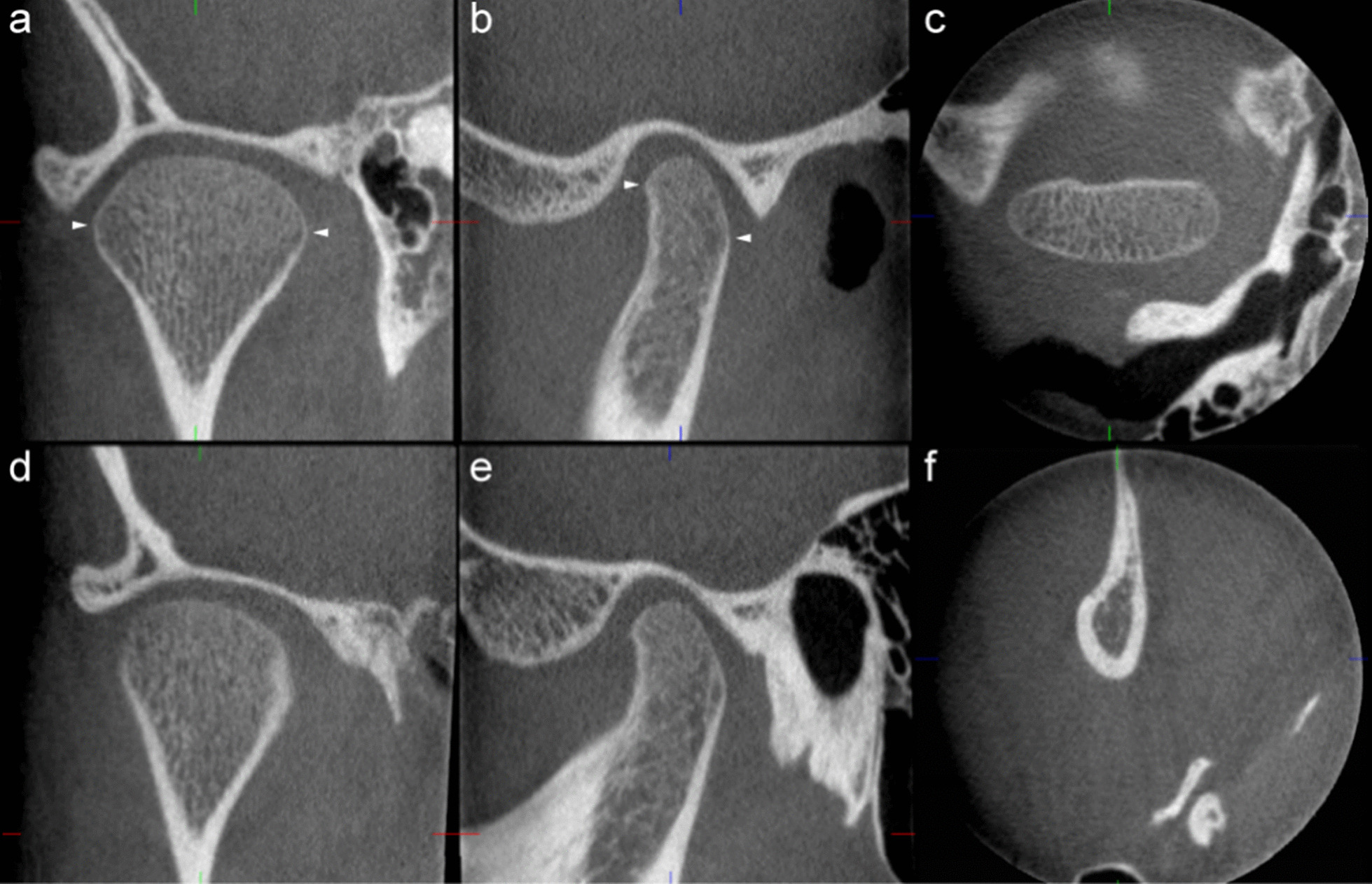
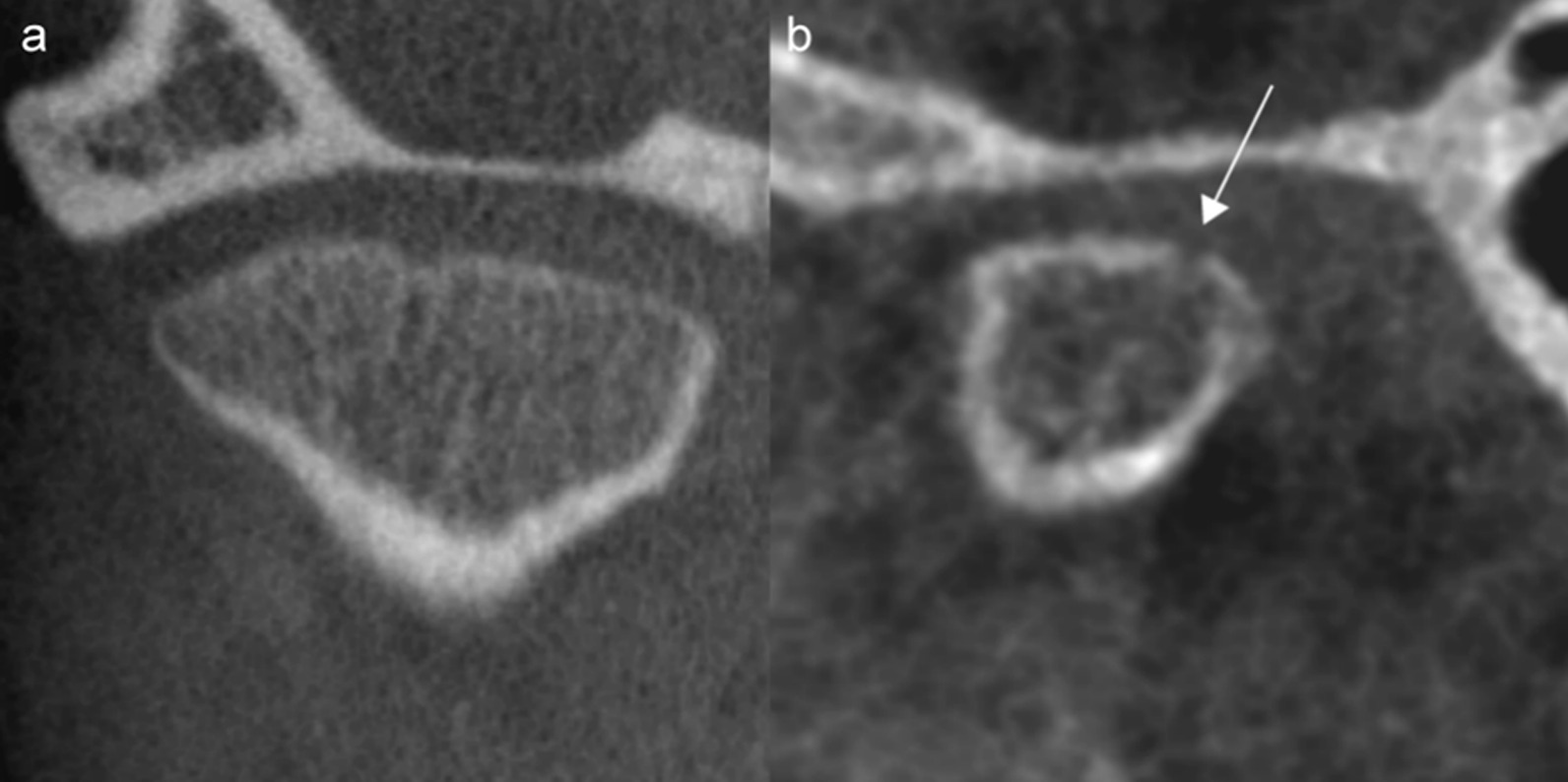
Background: The temporomandibular joint (TMJ) is frequently involved in juvenile idiopathic arthritis (JIA). Diagnostic imaging is necessary to correctly diagnose and evaluate TMJ involvement, however, hitherto little has been published on the accuracy of the applied scoring systems and measurements. The present study aims to investigate the precision of 20 imaging features and five measurements based on cone beam computed tomography (CBCT).
Methods: Imaging and clinical data from 84 participants in the Norwegian study on juvenile idiopathic arthritis, the NorJIA study, were collected. Altogether 20 imaging features and five measurements were evaluated independently by three experienced radiologists for intra- and interobserver agreement. Agreement of categorical variables was assessed by Fleiss', Cohen's simple or weighted Kappa as appropriate. Agreement of continuous variables was assessed with 95% limits of agreement as advised by Bland and Altman.
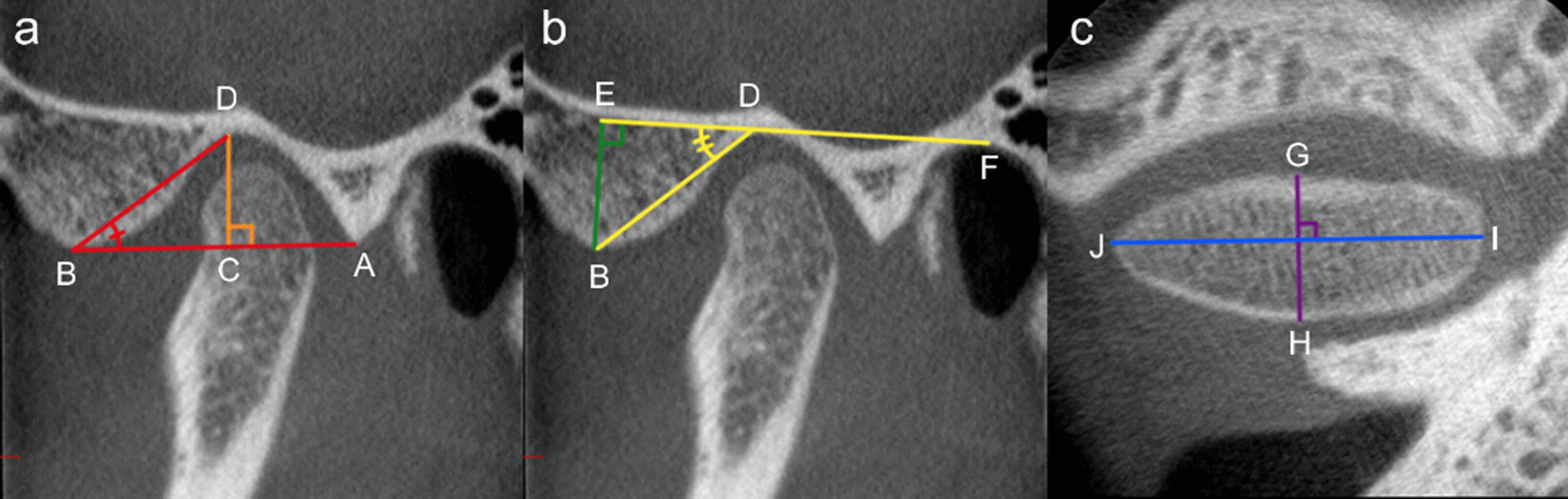
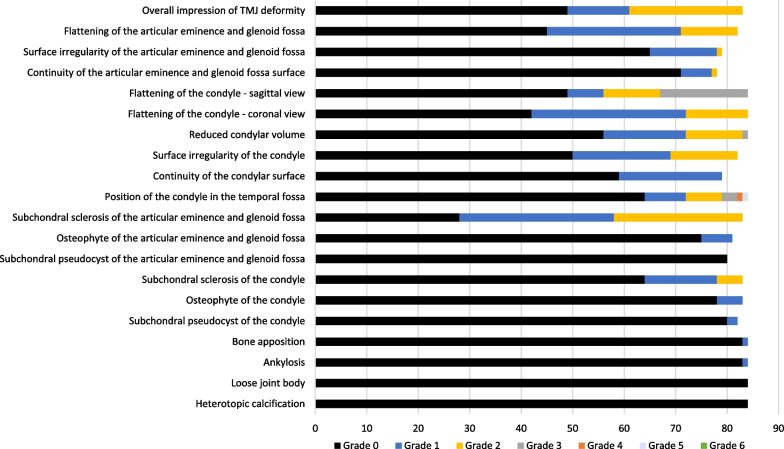
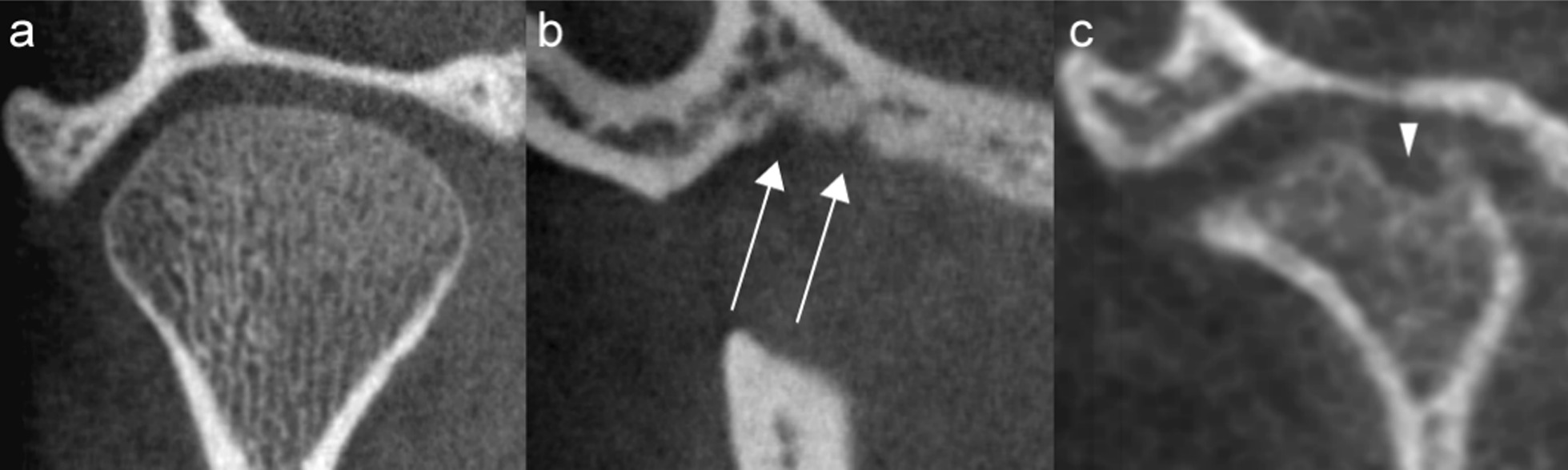
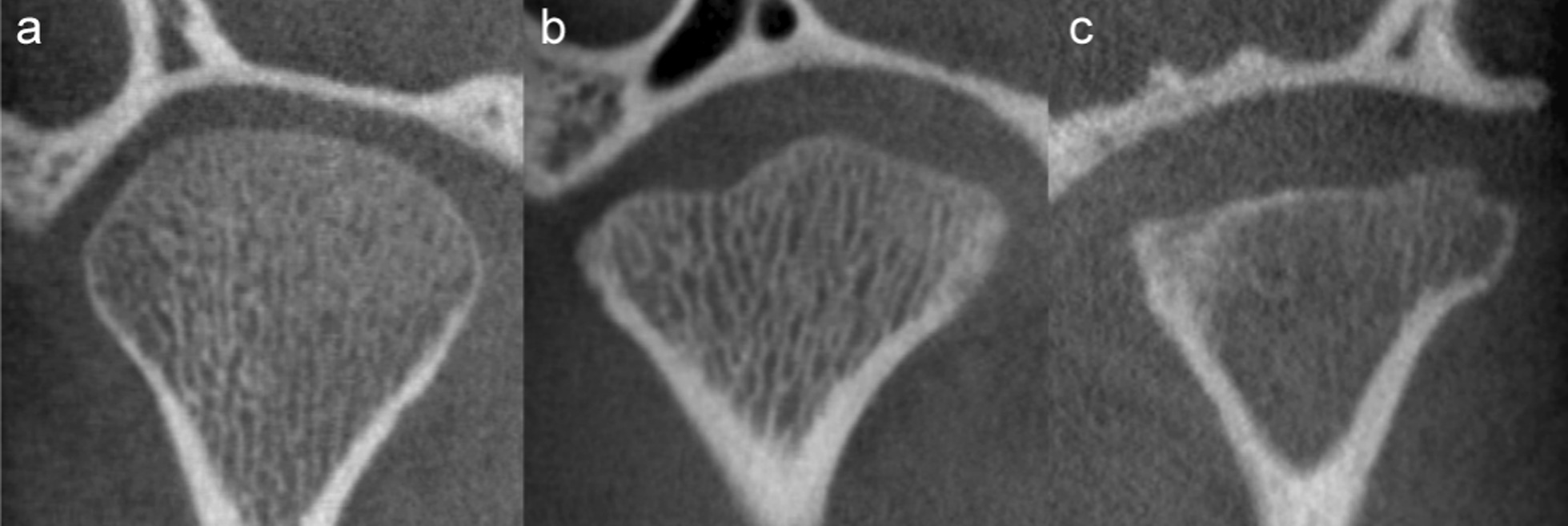
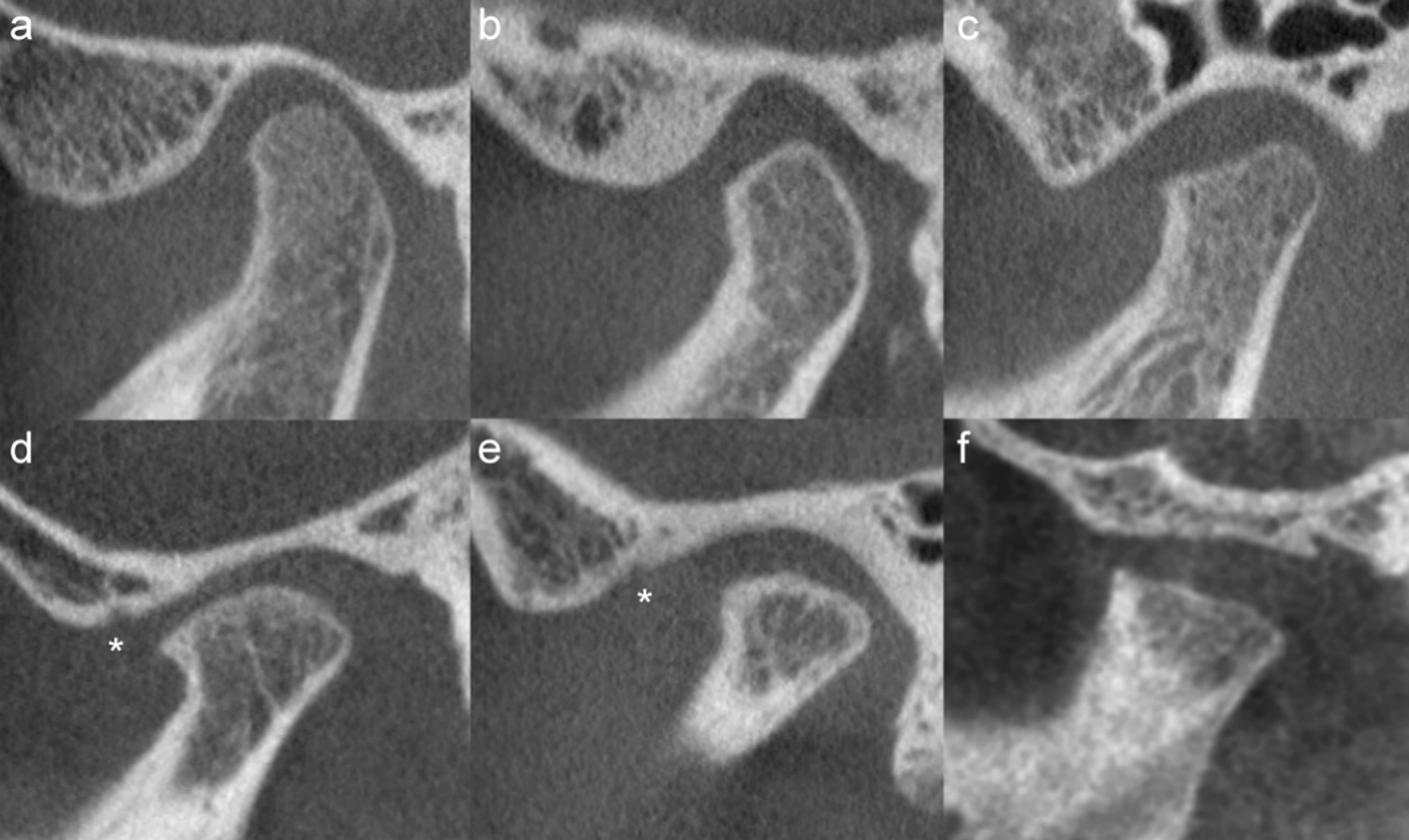
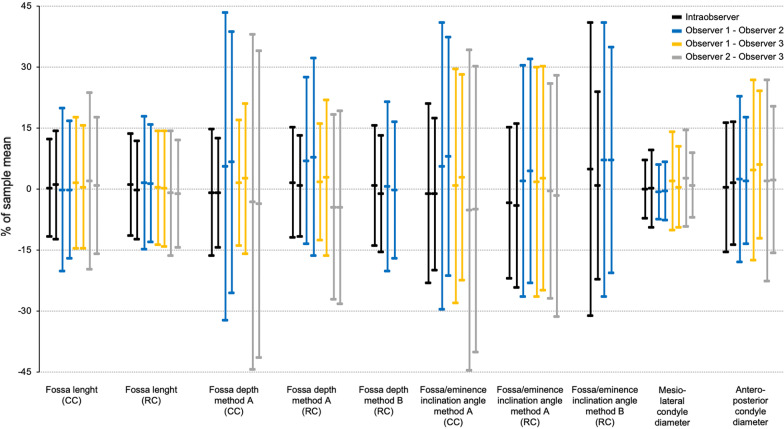
Results: "Overall impression of TMJ deformity" showed almost perfect intraobserver agreement with a kappa coefficient of 0.81 (95% CI 0.69-0.92), and substantial interobserver agreement (Fleiss' kappa 0.70 (0.61-0.78)). Moreover, both "flattening" and "irregularities" of the eminence/fossa and condyle performed well, with intra- and interobserver agreements of 0.66-0.82 and 0.55-0.76, respectively. "Reduced condylar volume" and "continuity" of the fossa/eminence had moderate intra- and interobserver Kappa values, whereas continuity of the condyle had Kappa values above 0.55. Measurements of distances and angles had limits of agreement of more than 15% of the sample mean.
Conclusions: We propose a CBCT-based scoring system of nine precise imaging features suggestive of TMJ deformity in JIA. Their clinical validity must be tested.
Trial registration: ClinicalTrials.gov NCT03904459.
Keywords: Arthritis juvenile; Observer variation; Precision; Scoring system; Temporomandibular joint.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
MRI in the Assessment of TMJ-Arthritis in Children with JIA; Repeatability of a Newly Devised Scoring System.Acad Radiol. 2022 Sep;29(9):1362-1377. doi: 10.1016/j.acra.2021.09.024. Epub 2021 Nov 19. Acad Radiol. 2022. PMID: 34802906
-
Observer agreement of imaging measurements used for evaluation of dentofacial deformity in juvenile idiopathic arthritis.Dentomaxillofac Radiol. 2022 Sep 1;51(6):20210478. doi: 10.1259/dmfr.20210478. Epub 2022 Aug 2. Dentomaxillofac Radiol. 2022. PMID: 35466687 Free PMC article.
-
In children and adolescents with temporomandibular disorder assembled with juvenile idiopathic arthritis - no association were found between pain and TMJ deformities using CBCT.BMC Oral Health. 2021 Oct 12;21(1):518. doi: 10.1186/s12903-021-01870-z. BMC Oral Health. 2021. PMID: 34641860 Free PMC article.
-
What is the image appearance of juvenile idiopathic arthritis in MRI, CT, and CBCT of TMJ? A systematic review.Clin Oral Investig. 2023 May;27(5):2321-2333. doi: 10.1007/s00784-022-04828-9. Epub 2022 Dec 14. Clin Oral Investig. 2023. PMID: 36515761
-
MR Imaging of the Temporomandibular Joint in Juvenile Idiopathic Arthritis: Technique and Findings.Radiographics. 2017 Mar-Apr;37(2):595-612. doi: 10.1148/rg.2017160078. Radiographics. 2017. PMID: 28287946 Review.
Cited by
-
Angular assessment of joints in juvenile idiopathic arthritis.Rheumatol Immunol Res. 2025 Apr 2;6(1):1-6. doi: 10.1515/rir-2025-0001. eCollection 2025 Mar. Rheumatol Immunol Res. 2025. PMID: 40191468 Free PMC article.
-
Cytokines in saliva, serum, and temporomandibular joint synovial fluid in children with juvenile idiopathic arthritis: An explorative cross-sectional study.Pediatr Rheumatol Online J. 2025 Jun 17;23(1):66. doi: 10.1186/s12969-025-01118-y. Pediatr Rheumatol Online J. 2025. PMID: 40528176 Free PMC article.
-
Image quality-based dose optimization in pediatric cone-beam computed tomography: A pilot methodological study.Imaging Sci Dent. 2024 Sep;54(3):264-270. doi: 10.5624/isd.20240030. Epub 2024 Jul 2. Imaging Sci Dent. 2024. PMID: 39371303 Free PMC article.
References
-
- Glerup M, Stoustrup P, Matzen LH, Rypdal V, Nordal E, Frid P, Arnstad ED, Rygg M, Thorarensen O, Ekelund M, et al. Longterm outcomes of temporomandibular joints in juvenile idiopathic arthritis: 17 years of followup of a nordic juvenile idiopathic arthritis cohort. J Rheumatol. 2020;47(5):730–738. doi: 10.3899/jrheum.190231. - DOI - PubMed
-
- Billiau AD, Hu Y, Verdonck A, Carels C, Wouters C. Temporomandibular joint arthritis in juvenile idiopathic arthritis: prevalence, clinical and radiological signs, and relation to dentofacial morphology. J Rheumatol. 2007;34(9):1925–1933. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
