

Real-World Effectiveness of Sotrovimab for the Early Treatment of COVID-19 During SARS-CoV-2 Delta and Omicron Waves in the USA
- PMID: 36629998
- PMCID: PMC9832411
- DOI: 10.1007/s40121-022-00755-0
Real-World Effectiveness of Sotrovimab for the Early Treatment of COVID-19 During SARS-CoV-2 Delta and Omicron Waves in the USA
Abstract
Introduction: Sotrovimab, a recombinant human monoclonal antibody (mAb) against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) had US Food and Drug Administration Emergency Use Authorization for the treatment of high-risk outpatients with mild-to-moderate coronavirus disease 2019 (COVID-19) from 26 May 2021 to 5 April 2022. Real-world clinical effectiveness of sotrovimab in reducing the risk of 30-day all-cause hospitalization and/or mortality was evaluated for the period when the prevalence of circulating SARS-CoV-2 variants changed between Delta and Omicron in the USA.
Methods: A retrospective analysis was conducted of de-identified patients diagnosed with COVID-19 between 1 September 2021 to 30 April 2022 in the FAIR Health National Private Insurance Claims database. Patients meeting high-risk criteria were divided into two cohorts: sotrovimab and not treated with a mAb ("no mAb"). All-cause hospitalizations and facility-reported mortality ≤ 30 days of diagnosis ("30-day hospitalization or mortality") were identified. Multivariable and propensity score-matched Poisson and logistic regressions were conducted to estimate the adjusted relative risk (RR) and odds of 30-day hospitalization or mortality in each cohort.
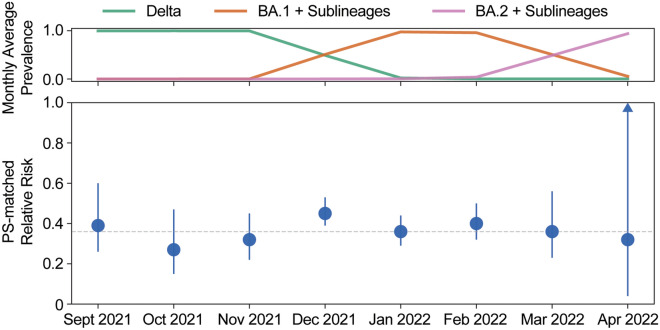
Results: Compared with the no mAb cohort (n = 1,514,868), the sotrovimab cohort (n = 15,633) was older and had a higher proportion of patients with high-risk conditions. In the no mAb cohort, 84,307 (5.57%) patients were hospitalized and 8167 (0.54%) deaths were identified, while in the sotrovimab cohort, 418 (2.67%) patients were hospitalized and 13 (0.08%) deaths were identified. After adjusting for potential confounders, the sotrovimab cohort had a 55% lower risk of 30-day hospitalization or mortality (RR 0.45, 95% CI 0.41-0.49) and an 85% lower risk of 30-day mortality (RR 0.15, 95% CI 0.08-0.29). Monthly, from September 2021 to April 2022, the RR reduction for 30-day hospitalization or mortality in the sotrovimab cohort was maintained, ranging from 46% to 71% compared with the no mAb cohort; the RR estimate in April 2022 was uncertain, with wide confidence intervals due to the small sample size.
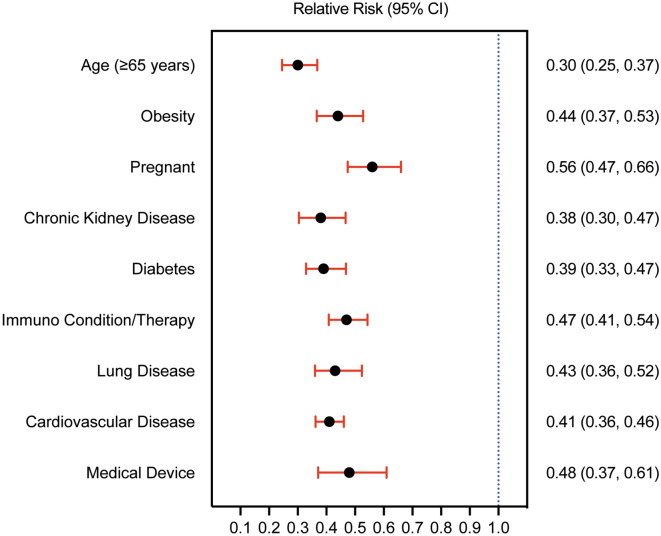
Conclusion: Sotrovimab was associated with reduced risk of 30-day all-cause hospitalization and mortality versus no mAb treatment. Clinical effectiveness persisted during Delta and early Omicron variant waves and among all high-risk subgroups assessed.
Keywords: COVID-19; Effectiveness; Monoclonal antibody; Real-world; SARS-CoV-2; Sotrovimab.
© 2023. The Author(s).
Figures
References
-
- World Health Organization. Coronavirus (COVID-19) Dashboard. https://covid19.who.int/. Accessed 22 Sep 2022.
-
- Coronavirus (COVID-19) Update: FDA Authorizes Additional Monoclonal Antibody for Treatment of COVID-19. News Release. FDA; May, 26, 2021. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19.... Accessed 20 May 2022.
LinkOut - more resources
Full Text Sources
Miscellaneous
