

Improving Risk Stratification for Patients With Type 2 Myocardial Infarction
- PMID: 36631210
- PMCID: PMC9841577
- DOI: 10.1016/j.jacc.2022.10.025
Improving Risk Stratification for Patients With Type 2 Myocardial Infarction
Abstract
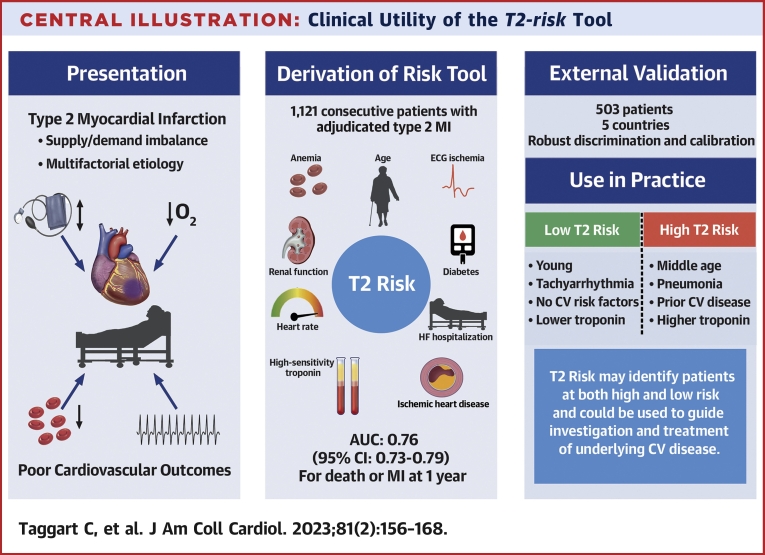
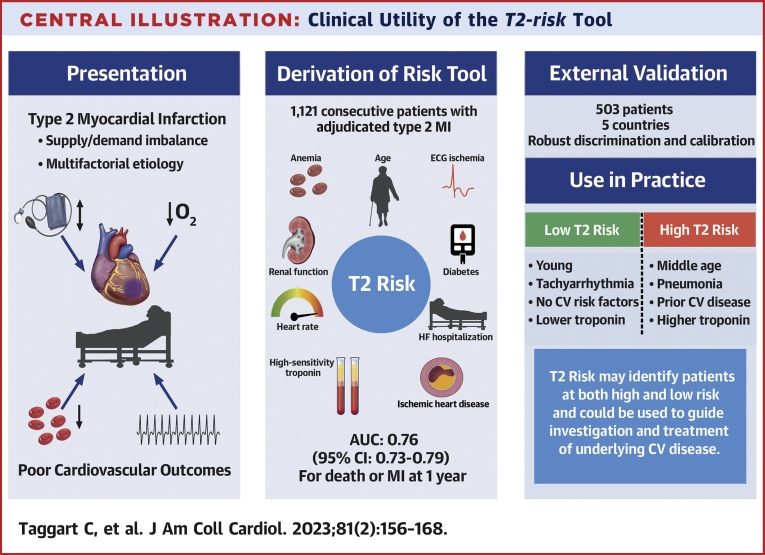
Background: Despite poor cardiovascular outcomes, there are no dedicated, validated risk stratification tools to guide investigation or treatment in type 2 myocardial infarction.
Objectives: The goal of this study was to derive and validate a risk stratification tool for the prediction of death or future myocardial infarction in patients with type 2 myocardial infarction.
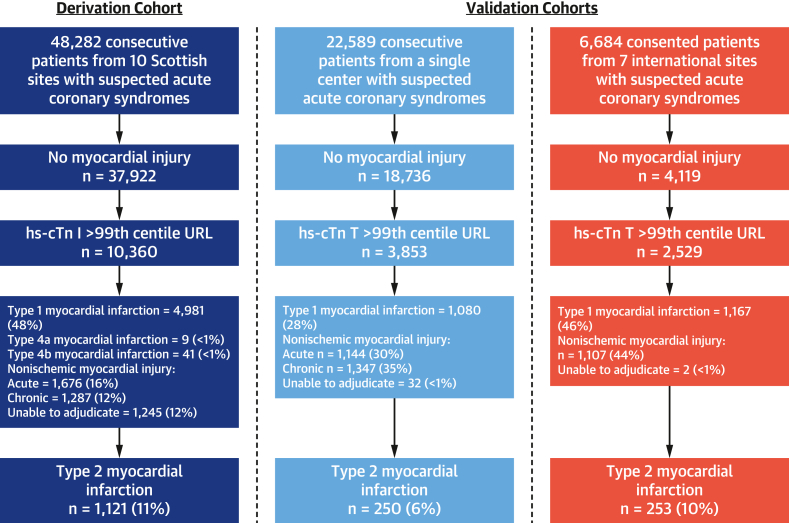
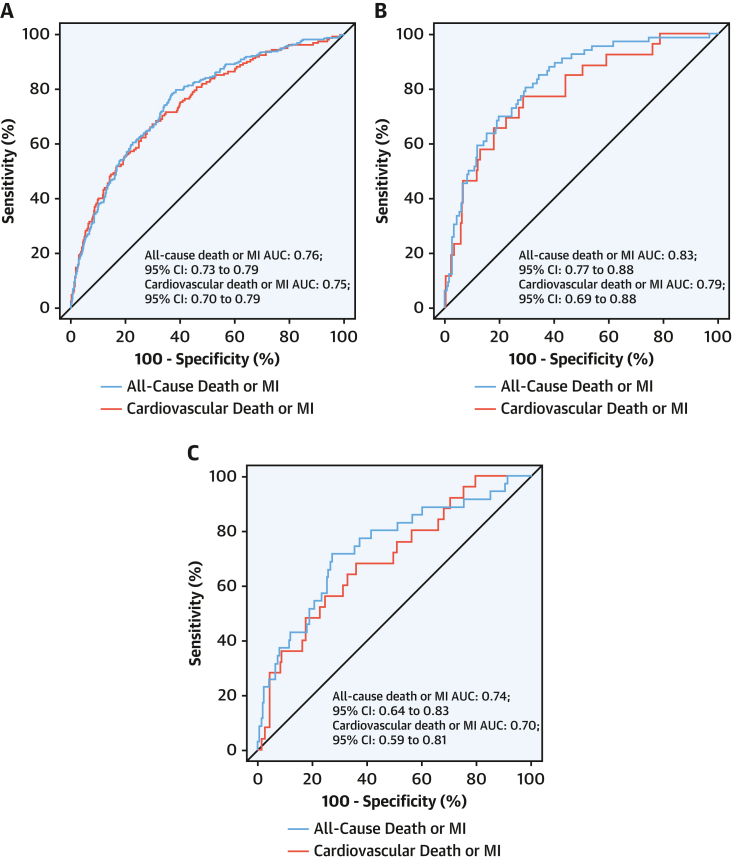
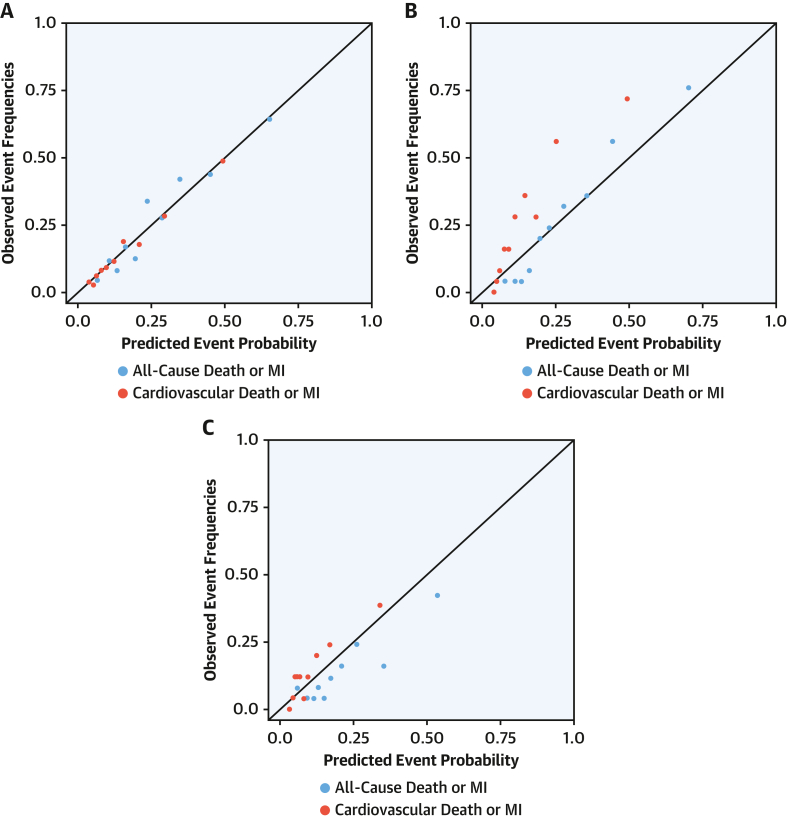
Methods: The T2-risk score was developed in a prospective multicenter cohort of consecutive patients with type 2 myocardial infarction. Cox proportional hazards models were constructed for the primary outcome of myocardial infarction or death at 1 year using variables selected a priori based on clinical importance. Discrimination was assessed by area under the receiving-operating characteristic curve (AUC). Calibration was investigated graphically. The tool was validated in a single-center cohort of consecutive patients and in a multicenter cohort study from sites across Europe.
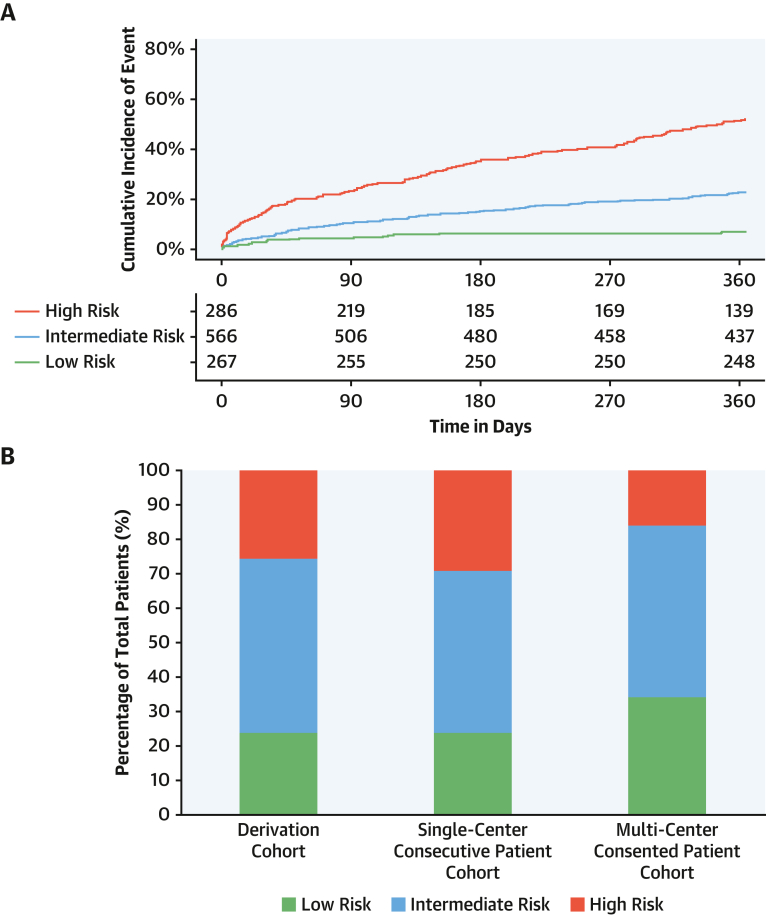
Results: There were 1,121, 250, and 253 patients in the derivation, single-center, and multicenter validation cohorts, with the primary outcome occurring in 27% (297 of 1,121), 26% (66 of 250), and 14% (35 of 253) of patients, respectively. The T2-risk score incorporating age, ischemic heart disease, heart failure, diabetes mellitus, myocardial ischemia on electrocardiogram, heart rate, anemia, estimated glomerular filtration rate, and maximal cardiac troponin concentration had good discrimination (AUC: 0.76; 95% CI: 0.73-0.79) for the primary outcome and was well calibrated. Discrimination was similar in the consecutive patient (AUC: 0.83; 95% CI: 0.77-0.88) and multicenter (AUC: 0.74; 95% CI: 0.64-0.83) cohorts. T2-risk provided improved discrimination over the Global Registry of Acute Coronary Events 2.0 risk score in all cohorts.
Conclusions: The T2-risk score performed well in different health care settings and could help clinicians to prognosticate, as well as target investigation and preventative therapies more effectively. (High-Sensitivity Troponin in the Evaluation of Patients With Suspected Acute Coronary Syndrome [High-STEACS]; NCT01852123).
Keywords: risk prediction; type 2 myocardial infarction.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This project was funded by a Starter Grant for Clinical Lecturers from the Academy of Medical Sciences (ARC; SGL021/1075). This work was also supported by DataLoch, which is funded by the Data Driven Innovation programme within the Edinburgh and Southeast Scotland City Region Deal. The High-STEACS trial was funded by a Special Project Grant (SP/12/10/29922) from the British Heart Foundation with assay reagent, calibrators, and controls provided by Abbott Laboratories without charge. Dr Taggart is supported by a British Heart Foundation Clinical Research Training Fellowship (FS/CRTF/21/2473). Dr Monterrubio-Gómez is supported by an MRC University Unit grant to the MRC Human Genetics Unit. Dr Vallejos is a Chancellor’s Fellow supported by the University of Edinburgh. Drs Wereski and Bularga are supported by Clinical Research Training Fellowships from the Medical Research Council (MR/V007017/1 and MR/V007254/1). Dr Mills is supported by a Chair Award, Programme Grant, Research Excellence Award (CH/F/21/90010, RG/20/10/34966, RE/18/5/34216), from the British Heart Foundation, Drs Vallejos and Mills are supported by a British Heart Foundation–Turing Cardiovascular Data Science Award (BCDSA/100003). Dr Mills has received honoraria or consultancy from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx. Dr Roos was supported by the Stockholm County Council (grant no. 20200935). Dr Boeddinghaus has received research grants from the University of Basel, the University Hospital of Basel and the Division of Internal Medicine, the Swiss Academy of Medical Sciences, the Gottfried and Julia Bangerter-Rhyner-Foundation, and the Swiss National Science Foundation; and has received speaker honoraria and/or consulting honoraria from Siemens, Roche, Ortho Clinical Diagnostics, and Quidel Corporation, outside of the submitted work.). Dr Nestelberger has received research support from the Swiss National Science Foundation (P400PM_191037/1), the Swiss Heart Foundation (FF20079), the Prof Dr Max Cloëtta Foundation, the Margarete und Walter Lichtenstein-Stiftung (3MS1038), the University of Basel, and the University Hospital Basel; and has received speaker honoraria/consulting honoraria from Siemens, Beckman Coulter, Bayer, Ortho Clinical Diagnostics, and Orion Pharma, all outside the submitted work. Dr Koechlin received a research grant from the Swiss Heart Foundation, the University of Basel, the Swiss Academy of Medical Sciences, and the Gottfried and Julia Bangerter-Rhyner Foundation, and the Freiwillige Akademische Gesellschaft Basel. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Type 2 Myocardial Infarction: Do We Need Risk Scores?J Am Coll Cardiol. 2023 Jan 17;81(2):169-171. doi: 10.1016/j.jacc.2022.11.010. J Am Coll Cardiol. 2023. PMID: 36631211 No abstract available.
-
In type 2 MI, the T2-risk score predicted death or MI at 1 y.Ann Intern Med. 2023 May;176(5):JC58. doi: 10.7326/J23-0027. Epub 2023 May 2. Ann Intern Med. 2023. PMID: 37267075
References
-
- Thygesen K., Alpert J.S., Jaffe A.S., et al. Fourth universal definition of myocardial infarction (2018) Eur Heart J. 2018;40:237–269. - PubMed
-
- Lambrecht S., Sarkisian L., Saaby L., Poulsen T.S., Thygesen K., Mickley H. Different causes of death in patients with myocardial infarction type 1, type 2, and myocardial injury. Am J Med. 2018;131:548–554. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- MR/W000598/1/MRC_/Medical Research Council/United Kingdom
- MR/V007254/1/MRC_/Medical Research Council/United Kingdom
- CH/F/21/90010/BHF_/British Heart Foundation/United Kingdom
- RG/20/10/34966/BHF_/British Heart Foundation/United Kingdom
- FS/CRTF/21/24273/BHF_/British Heart Foundation/United Kingdom
- MR/V007017/1/MRC_/Medical Research Council/United Kingdom
- SP/18/2/33800/BHF_/British Heart Foundation/United Kingdom
- FS/CRTF/21/2473/BHF_/British Heart Foundation/United Kingdom
- BCDSA/100003/BHF_/British Heart Foundation/United Kingdom
- SP/12/10/29922/BHF_/British Heart Foundation/United Kingdom
- RE/18/5/34216/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
