

Trends in inpatient and post-discharge mortality among young infants admitted to Kilifi County Hospital, Kenya: a retrospective cohort study
- PMID: 36631234
- PMCID: PMC9835934
- DOI: 10.1136/bmjopen-2022-067482
Trends in inpatient and post-discharge mortality among young infants admitted to Kilifi County Hospital, Kenya: a retrospective cohort study
Abstract
Objectives: To describe admission trends and estimate inpatient and post-discharge mortality and its associated exposures, among young infants (YI) admitted to a county hospital in Kenya.
Design: Retrospective cohort study.
Setting: Secondary level hospital.
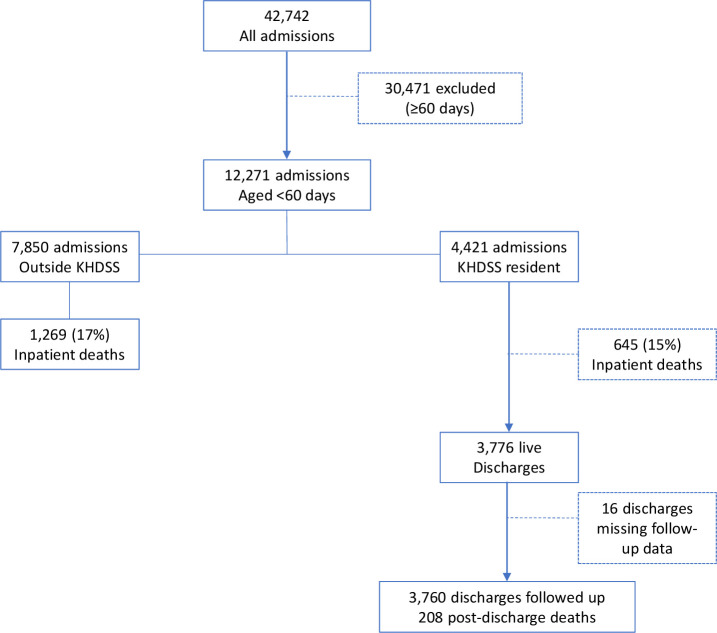
Participants: YI aged less than 60 days admitted to hospital from January 2009 to December 2019: 12 271 admissions in 11 877 individuals. YI who were resident within a Kilifi Health and Demographic Surveillance System (KHDSS): n=3625 with 4421 admissions were followed-up for 1 year after discharge.
Primary and secondary outcome measures: Inpatient and 1-year post-discharge mortality, the latter in KHDSS residents.
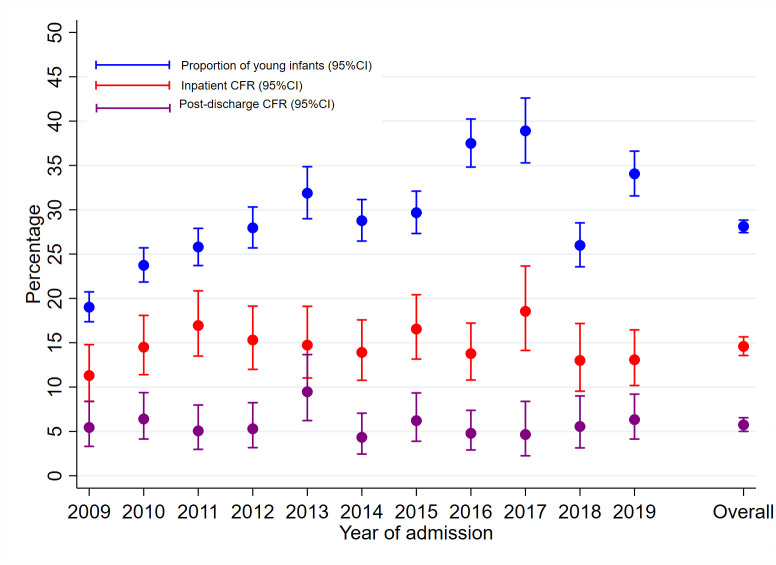
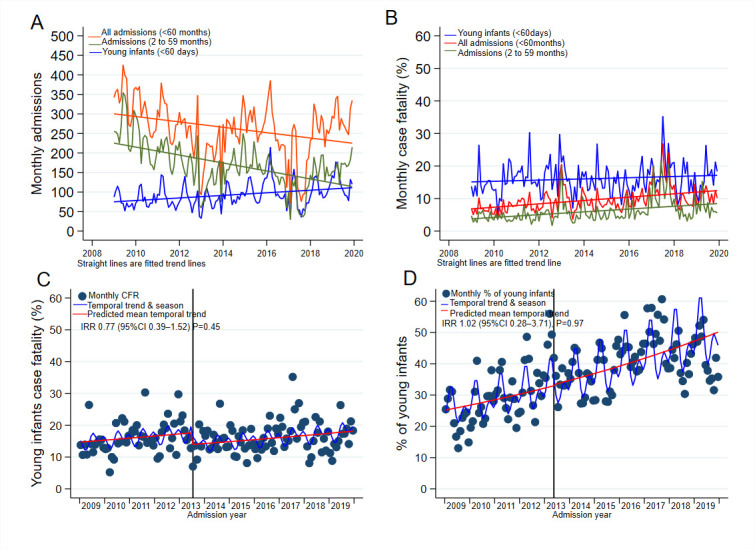
Results: Of 12 271 YI admissions, 4421 (36%) were KHDSS-resident. Neonatal sepsis, preterm complications and birth asphyxia accounted for 83% of the admissions. The proportion of YI among under-5s admissions increased from 19% in 2009 to 34% in 2019 (Ptrend=0.02). Inpatient case fatality was 16%, with 66% of the deaths occurring within 48 hours of admission. The introduction of free maternity care in 2013 was not associated with a change in admissions or inpatient mortality among YI. During 1-year post-discharge, 208/3625 (5.7%) YI died, 64.3 (95% CI 56.2 to 73.7) per 1000 infant-years. 49% of the post-discharge deaths occurred within 1 month of discharge, and 49% of post-discharge deaths occurred at home. Both inpatient and post-discharge deaths were associated with low admission weight. Inpatient mortality was associated with clinical signs of disease severity, while post-discharge mortality was associated with the length of hospitalisation, leaving against advice and referral to a specialised hospital.
Conclusions: YIs accounted for an increasing proportion of paediatric admissions and their overall mortality remains high. Post-discharge mortality accounts for a lower proportion of deaths but mortality rate is higher than among children aged 2-59 months. Services to address post-discharge mortality are needed and should focus on infants at higher risk.
Keywords: epidemiology; neonatology; paediatrics.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: JB declares the following: Chair of the DSMB for ‘Efficacy and safety of whole-body chlorhexidine cleansing in reducing bacterial skin colonisation of hospitalised neonates - a pilot trial’. St George’s, University of London and global sites; Treasurer of the Commonwealth Society for Paediatric Gastroenterology & Nutrition.
Figures
References
-
- UNICEF . Levels & Trends in Child Mortality: Report 2020, Estimates developed by the United Nations Inter-agency Group for Child Mortality Estimation. New York: United Nations Children’s Fund, 2020.
-
- GBD 2015 Child Mortality Collaborators . Global, regional, National, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet 2016;388:1725–74. 10.1016/S0140-6736(16)31575-6 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources