

CT-radiomics and clinical risk scores for response and overall survival prognostication in TACE HCC patients
- PMID: 36631548
- PMCID: PMC9834236
- DOI: 10.1038/s41598-023-27714-0
CT-radiomics and clinical risk scores for response and overall survival prognostication in TACE HCC patients
Abstract
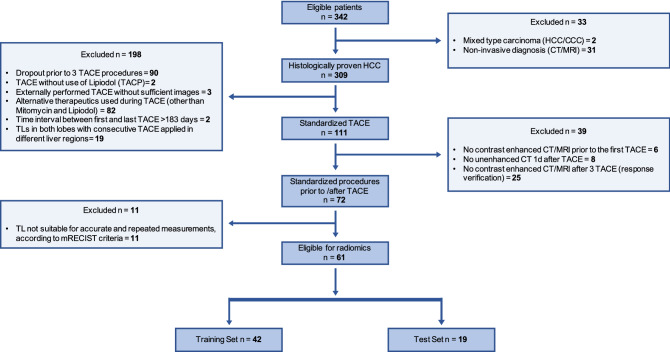
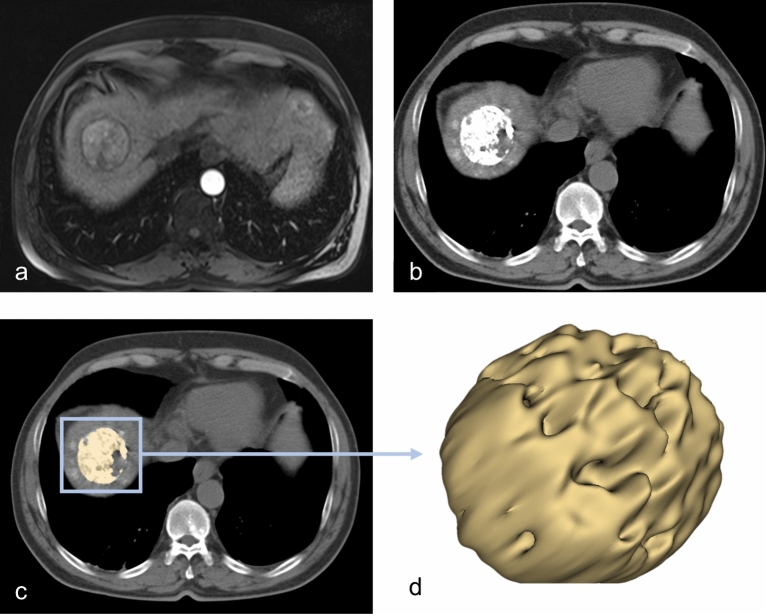
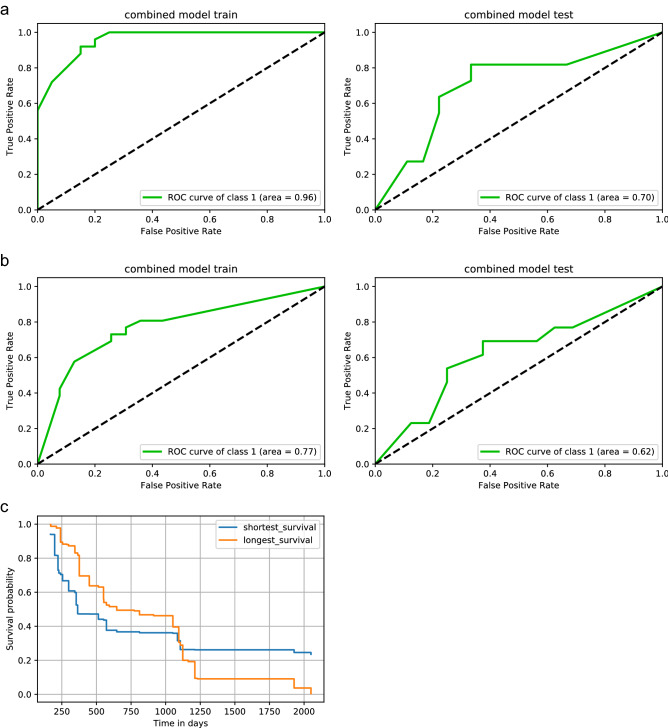
We aimed to identify hepatocellular carcinoma (HCC) patients who will respond to repetitive transarterial chemoembolization (TACE) to improve the treatment algorithm. Retrospectively, 61 patients (mean age, 65.3 years ± 10.0 [SD]; 49 men) with 94 HCC mRECIST target-lesions who had three consecutive TACE between 01/2012 and 01/2020 were included. Robust and non-redundant radiomics features were extracted from the 24 h post-embolization CT. Five different clinical TACE-scores were assessed. Seven different feature selection methods and machine learning models were used. Radiomics, clinical and combined models were built to predict response to TACE on a lesion-wise and patient-wise level as well as its impact on overall-survival prognostication. 29 target-lesions of 19 patients were evaluated in the test set. Response rates were 37.9% (11/29) on the lesion-level and 42.1% (8/19) on the patient-level. Radiomics top lesion-wise response prognostications was AUC 0.55-0.67. Clinical scores revealed top AUCs of 0.65-0.69. The best working model combined the radiomic feature LargeDependenceHighGrayLevelEmphasis and the clinical score mHAP_II_score_group with AUC = 0.70, accuracy = 0.72. We transferred this model on a patient-level to achieve AUC = 0.62, CI = 0.41-0.83. The two radiomics-clinical features revealed overall-survival prognostication of C-index = 0.67. In conclusion, a random forest model using the radiomic feature LargeDependenceHighGrayLevelEmphasis and the clinical mHAP-II-score-group seems promising for TACE response prognostication.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
