

Outcomes Following Adalimumab Bio-originator to Biosimilar Switch-A Comparison Using Real-world Patient- and Physician-Reported Data in European Countries
- PMID: 36631636
- PMCID: PMC9834672
- DOI: 10.1007/s40744-022-00526-w
Outcomes Following Adalimumab Bio-originator to Biosimilar Switch-A Comparison Using Real-world Patient- and Physician-Reported Data in European Countries
Abstract
Introduction: The aim of this work is to compare real-world outcomes of patients with rheumatoid arthritis (RA) receiving adalimumab (ADA) bio-originator (non-switchers) to those who had switched from ADA bio-originator to an ADA biosimilar (switchers) on the basis of the hypothesis that these outcomes would differ.
Methods: Data were drawn from the Adelphi RA Disease Specific Programme™, a point-in-time survey of physicians and their patients in Europe (France, Germany, Italy, Spain, UK) in 2020. Physicians completed a questionnaire for their next ten adult patients with RA, followed by four additional patients who had switched from ADA bio-originator to an ADA biosimilar (switchers). Physician- and patient-reported outcomes (PROs) for switchers and non-switchers were compared by propensity score matching.
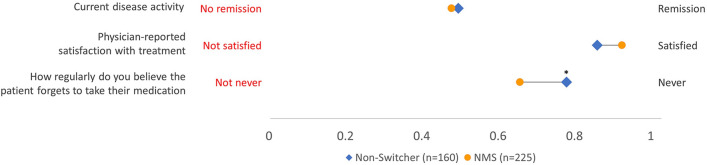
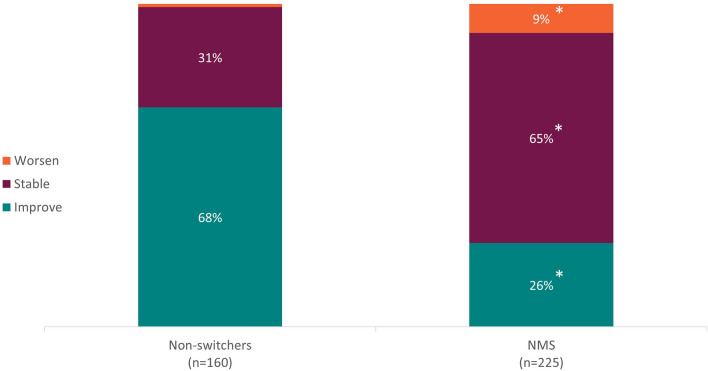
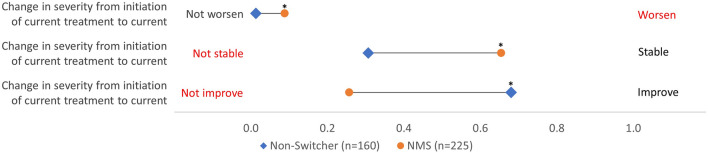
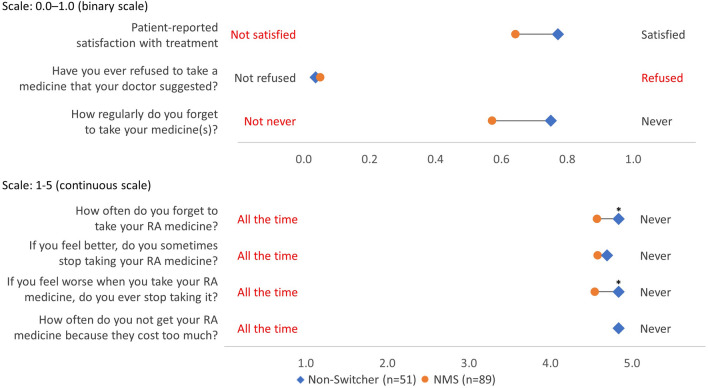
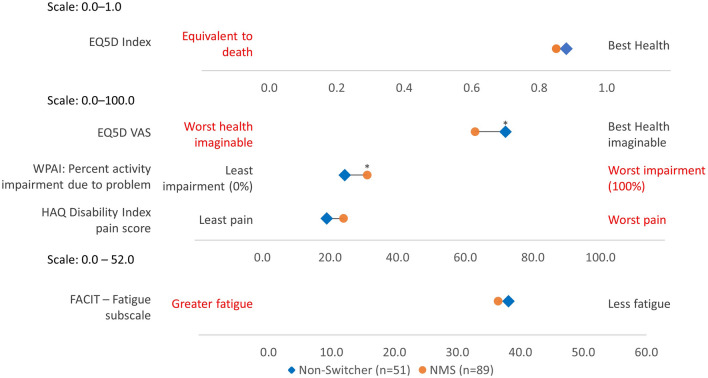
Results: Three hundred and three rheumatologists provided data for 160 non-switchers and 225 switchers, 140 patients provided data; 51 non-switchers, 89 switchers. According to physician-reported disease activity, non-switchers were more likely to improve on their current ADA treatment than switchers (68%, n = 108 vs. 26%, n = 59 p < 0.001) and less likely to worsen (1%, n = 2 vs. 9%, n = 20; p < 0.01). Physician-reported patient adherence was significantly lower amongst switchers versus non-switchers (0.66 vs. 0.78, respectively; p = 0.04). More non-switchers than switchers were reported by their physicians to be consistent in taking their RA medicine (p < 0.001). Compared with non-switchers, PRO measures indicated quality of life was worse (EQ-5D Visual Analogue Scale: 62.9 vs. 71.9; p < 0.001) and activity impairment was greater (Work Productivity Activity Index: 31.0 vs. 24.4; p = 0.02) for switchers, with trends for poorer health status and greater pain.
Conclusions: Non-medical switching in RA treatment may lead to unforeseen outcomes that should be considered by health decision-makers.
Keywords: Adalimumab; Biosimilar; Disease burden; Non-medical switching; Rheumatoid arthritis.
© 2023. The Author(s).
Figures
References
-
- Smolen JS, Landewé RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi: 10.1136/annrheumdis-2019-216655. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
