

Machine learning for predicting neurodegenerative diseases in the general older population: a cohort study
- PMID: 36631766
- PMCID: PMC9832793
- DOI: 10.1186/s12874-023-01837-4
Machine learning for predicting neurodegenerative diseases in the general older population: a cohort study
Erratum in
-
Correction: Machine learning for predicting neurodegenerative diseases in the general older population: a cohort study.BMC Med Res Methodol. 2023 Jan 31;23(1):32. doi: 10.1186/s12874-023-01854-3. BMC Med Res Methodol. 2023. PMID: 36721092 Free PMC article. No abstract available.
Abstract
Background: In the older general population, neurodegenerative diseases (NDs) are associated with increased disability, decreased physical and cognitive function. Detecting risk factors can help implement prevention measures. Using deep neural networks (DNNs), a machine-learning algorithm could be an alternative to Cox regression in tabular datasets with many predictive features. We aimed to compare the performance of different types of DNNs with regularized Cox proportional hazards models to predict NDs in the older general population.
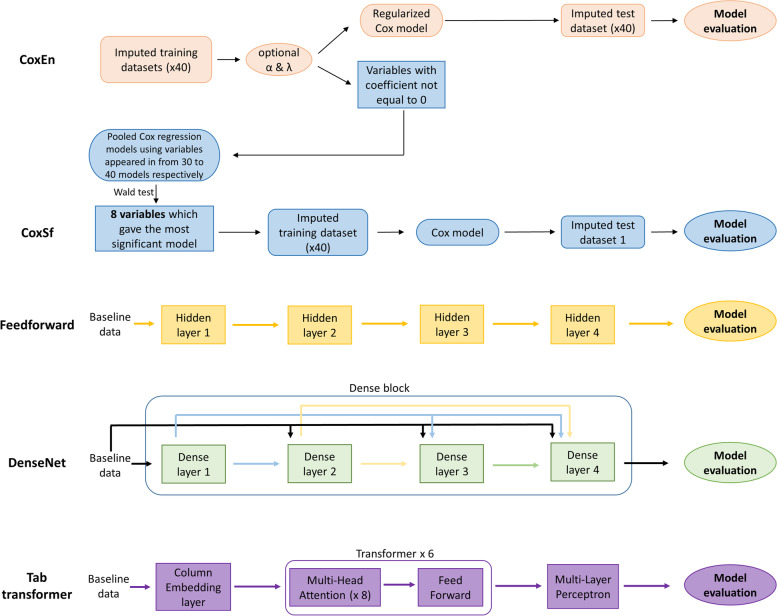
Methods: We performed a longitudinal analysis with participants of the English Longitudinal Study of Ageing. We included men and women with no NDs at baseline, aged 60 years and older, assessed every 2 years from 2004 to 2005 (wave2) to 2016-2017 (wave 8). The features were a set of 91 epidemiological and clinical baseline variables. The outcome was new events of Parkinson's, Alzheimer or dementia. After applying multiple imputations, we trained three DNN algorithms: Feedforward, TabTransformer, and Dense Convolutional (Densenet). In addition, we trained two algorithms based on Cox models: Elastic Net regularization (CoxEn) and selected features (CoxSf).
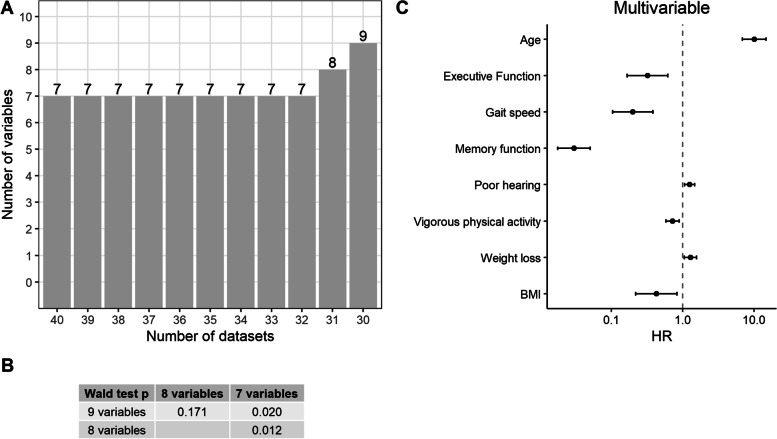
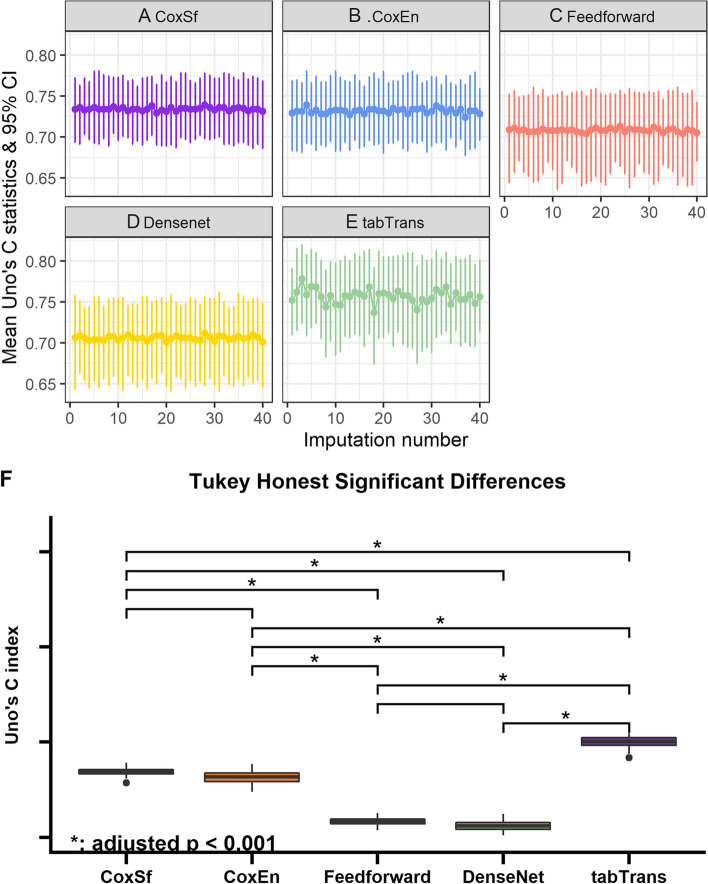
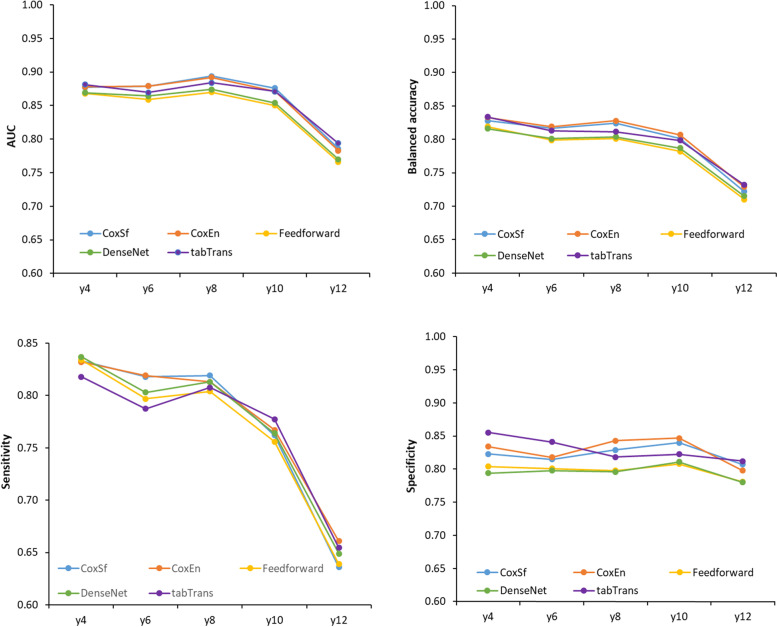
Results: 5433 participants were included in wave 2. During follow-up, 12.7% participants developed NDs. Although the five models predicted NDs events, the discriminative ability was superior using TabTransformer (Uno's C-statistic (coefficient (95% confidence intervals)) 0.757 (0.702, 0.805). TabTransformer showed superior time-dependent balanced accuracy (0.834 (0.779, 0.889)) and specificity (0.855 (0.0.773, 0.909)) than the other models. With the CoxSf (hazard ratio (95% confidence intervals)), age (10.0 (6.9, 14.7)), poor hearing (1.3 (1.1, 1.5)) and weight loss 1.3 (1.1, 1.6)) were associated with a higher DNN risk. In contrast, executive function (0.3 (0.2, 0.6)), memory (0, 0, 0.1)), increased gait speed (0.2, (0.1, 0.4)), vigorous physical activity (0.7, 0.6, 0.9)) and higher BMI (0.4 (0.2, 0.8)) were associated with a lower DNN risk.
Conclusion: TabTransformer is promising for prediction of NDs with heterogeneous tabular datasets with numerous features. Moreover, it can handle censored data. However, Cox models perform well and are easier to interpret than DNNs. Therefore, they are still a good choice for NDs.
Keywords: Alzheimer; Cox models; Deep neural networks; Dementia; Older general population; Parkinson disease; Prediction; Tabular data.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
