

Confusion and prospects for carcinogenesis of gastric adenoma and dysplasia: What is the correct answer currently?
- PMID: 36632315
- PMCID: PMC9827587
- DOI: 10.3748/wjg.v28.i48.6900
Confusion and prospects for carcinogenesis of gastric adenoma and dysplasia: What is the correct answer currently?
Abstract
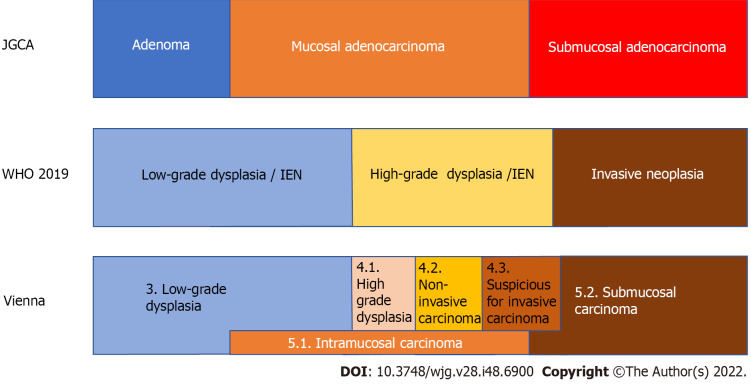
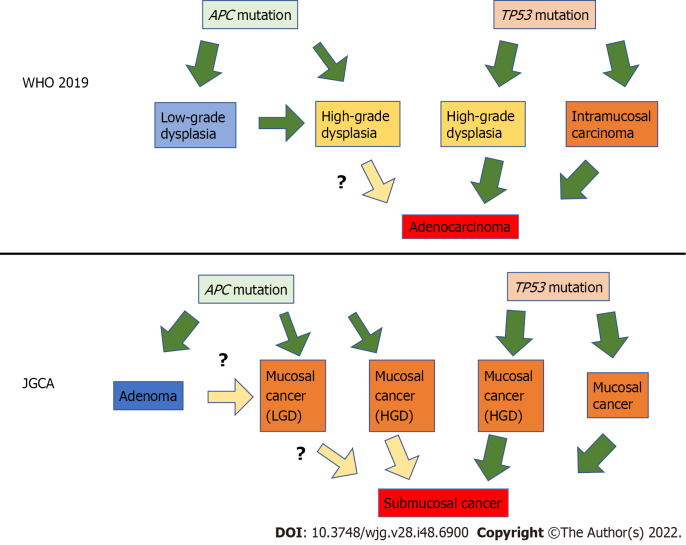
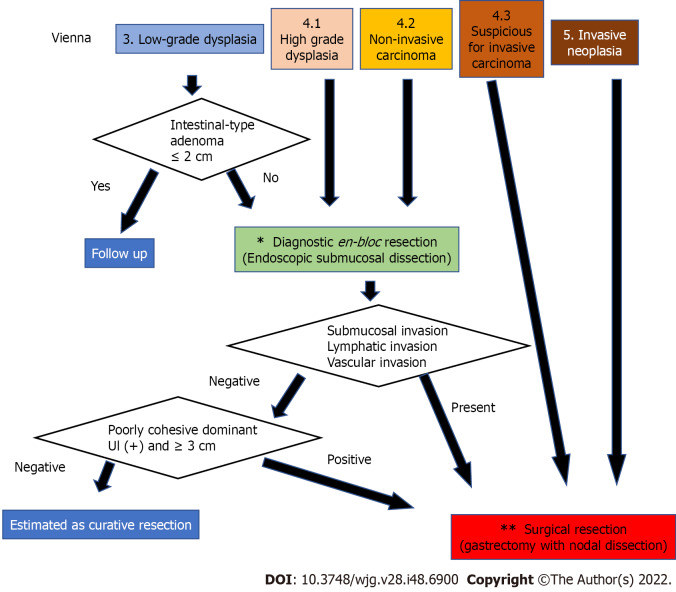
There are differences in the diagnoses of superficial gastric lesions between Japan and other countries. In Japan, superficial gastric lesions are classified as adenoma or cancer. Conversely, outside Japan, the same lesion is classified as low-grade dysplasia (LGD), high-grade dysplasia, or invasive neoplasia. Gastric carcinogenesis occurs mostly de novo, and the adenoma-carcinoma sequence does not appear to be the main pathway of carcinogenesis. Superficial gastric tumors can be roughly divided into the APC mutation type and the TP53 mutation type, which are mutually exclusive. APC-type tumors have low malignancy and develop into LGD, whereas TP53-type tumors have high malignancy and are considered cancerous even if small. For lesions diagnosed as category 3 or 4 in the Vienna classification, it is desirable to perform complete en bloc resection by endoscopic submucosal dissection followed by staging. If there is lymphovascular or submucosal invasion after mucosal resection, additional surgical treatment of gastrectomy with lymph node dissection is required. In such cases, function-preserving curative gastrectomy guided by sentinel lymph node biopsy may be a good alternative.
Keywords: Endoscopic submucosal dissection; Gastric adenoma; High-grade dysplasia; Intramucosal carcinoma; Low-grade dysplasia; Submucosal carcinoma.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflict of interest related to the publication of this study.
Figures
References
-
- Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S, Yamakido M, Taniyama K, Sasaki N, Schlemper RJ. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001;345:784–789. - PubMed
-
- Ueda J, Gosho M, Inui Y, Matsuda T, Sakakibara M, Mabe K, Nakajima S, Shimoyama T, Yasuda M, Kawai T, Murakami K, Kamada T, Mizuno M, Kikuchi S, Lin Y, Kato M. Prevalence of Helicobacter pylori infection by birth year and geographic area in Japan. Helicobacter. 2014;19:105–110. - PubMed
-
- Maddineni G, Xie JJ, Brahmbhatt B, Mutha P. Diet and carcinogenesis of gastric cancer. Curr Opin Gastroenterol. 2022;38:588–591. - PubMed
-
- Bornschein J, Malfertheiner P. Gastric carcinogenesis. Langenbecks Arch Surg. 2011;396:729–742. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
