

Impact of hematopoietic stem cell transplantation in glycogen storage disease type Ib: A single-subject research design using 13C-glucose breath test
- PMID: 36632325
- PMCID: PMC9826966
- DOI: 10.1016/j.ymgmr.2023.100955
Impact of hematopoietic stem cell transplantation in glycogen storage disease type Ib: A single-subject research design using 13C-glucose breath test
Abstract
Background: Glycogen storage disease type Ib (GSD Ib) is an autosomal recessively inherited deficiency of the glucose-6-phosphate translocase (G6PT). Clinical features include a combination of a metabolic phenotype (fasting hypoglycemia, lactic acidosis, hepatomegaly) and a hematologic phenotype with neutropenia and neutrophil dysfunction. Dietary treatment involves provision of starches such as uncooked cornstarch (UCCS) and Glycosade® to provide prolonged enteral supply of glucose. Granulocyte colony-stimulating factor (G-CSF) is the treatment of choice for neutropenia. Because long-term stimulation of hematopoiesis with G-CSF causes serious complications such as splenomegaly, hypersplenism, and osteopenia; hematopoietic stem cell transplantation (HSCT) has been considered in some patients with GSD Ib to correct neutropenia and avoid G-CSF related adverse effects. Whether HSCT also has an effect on the metabolic phenotype and utilization of carbohydrate sources has not been determined.
Objective: Our objective was to measure the utilization of starch in a patient with GSD Ib before and after HSCT using the minimally invasive 13C-glucose breath test (13C-GBT).
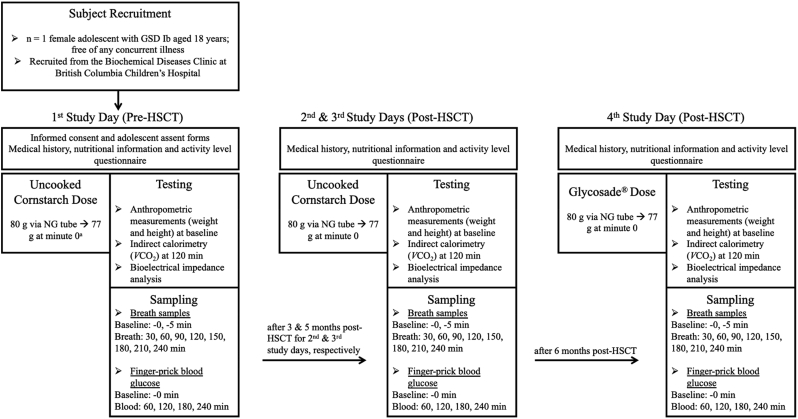
Design: A case of GSD Ib (18y; female) underwent 13C-GBT four times: UCCS (pre-HSCT), UCCS (3, 5 months post-HSCT) and Glycosade® (6 months post-HSCT) with a dose of 80 g administered via nasogastric tube after a 4 h fast according to our patient's fasting tolerance. Breath samples were collected at baseline and every 30 min for 240 min. Rate of CO2 production was measured at 120 min using indirect calorimetry. Finger-prick blood glucose was measured using a glucometer hourly to test hypoglycemia (glucose <4 mmol/L). Biochemical and clinical data were obtained from the medical records as a post-hoc chart review.
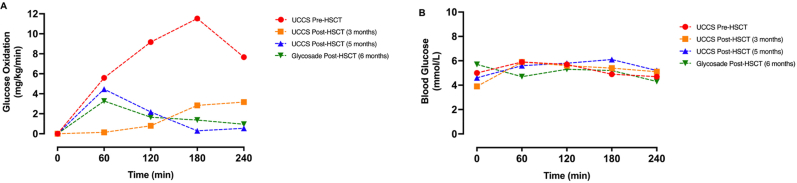
Results: UCCS utilization was significantly higher in GSD Ib pre-HSCT, which reduced and stabilized 5 months post-HSCT. UCCS and Glycosade® utilizations were low and not different at 5 and 6 months post-HSCT. Blood glucose concentrations were not significantly different at any time point.
Conclusions: Findings show that HSCT stabilized UCCS utilization, as reflected by lower and stable glucose oxidation. The results also illustrate the application of 13C-GBT to examine glucose metabolism in response to various carbohydrate sources after other treatment modalities like HSCT in GSD Ib.
Keywords: 13C-GBT, 13C-glucose breath test; 13C-glucose; ALT, alanine aminotransferase; AML, acute myeloid leukemia; ANOVA, analysis of variance; AST, aspartate aminotransferase; AUC, area under the curve; BIA, bioelectrical impedance analysis; BMI, body mass index; Breath test; CF-IRMS, continuous flow isotope ratio mass spectrometer; CGM, continuous glucose monitor; CRP, C-reactive protein; Cmax, maximum peak enrichment in 13CO2 oxidation; ER, endoplasmic reticulum; FFM, fat free mass; FM, fat mass; G-CSF, granulocyte colony-stimulating factor; G6P, glucose-6-phosphate; G6PT, glucose-6-phosphate translocase; G6Pase-ß, glucose-6-phosphatase-β; G6Pase-α, glucose-6-phosphatase-α; GGT, gamma glutamyltransferase; GSD I, glycogen storage disease type I; GSD III, glycogen storage disease type III; GSD Ia, glycogen storage disease type Ia; GSD Ib, glycogen storage disease type Ib; Glycogen storage disease type Ib; Glycosade®; HSCT/BMT, hematopoietic stem cell transplantation / bone marrow transplantation; Hematopoietic stem cell transplantation; IBD, inflammatory bowel disease; IM, intramuscular; NG, nasogastric; TBW, total body water; UCCS, uncooked cornstarch; Uncooked cornstarch; VCO2, rate of carbon dioxide production.; tmax, time to reach maximum 13CO2 oxidation.
© 2023 The Author(s).
Conflict of interest statement
None.
Figures
Similar articles
-
Development of minimally invasive 13C-glucose breath test to examine different exogenous carbohydrate sources in patients with glycogen storage disease type Ia.Mol Genet Metab Rep. 2022 May 11;31:100880. doi: 10.1016/j.ymgmr.2022.100880. eCollection 2022 Jun. Mol Genet Metab Rep. 2022. PMID: 35585965 Free PMC article.
-
Type I glycogen storage diseases: disorders of the glucose-6-phosphatase/glucose-6-phosphate transporter complexes.J Inherit Metab Dis. 2015 May;38(3):511-9. doi: 10.1007/s10545-014-9772-x. Epub 2014 Oct 7. J Inherit Metab Dis. 2015. PMID: 25288127 Review.
-
Glycogen Storage Disease Type III.2010 Mar 9 [updated 2022 Jan 6]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2010 Mar 9 [updated 2022 Jan 6]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 20301788 Free Books & Documents. Review.
-
Glycogen storage disease type I and G6Pase-β deficiency: etiology and therapy.Nat Rev Endocrinol. 2010 Dec;6(12):676-88. doi: 10.1038/nrendo.2010.189. Epub 2010 Oct 26. Nat Rev Endocrinol. 2010. PMID: 20975743 Free PMC article. Review.
-
Utilization of cornstarch in glycogen storage disease type Ia.Eur J Gastroenterol Hepatol. 2002 Nov;14(11):1251-6. doi: 10.1097/00042737-200211000-00014. Eur J Gastroenterol Hepatol. 2002. PMID: 12439121
References
-
- Annabi B., Mansfield B.C., Hiraiwa H., Lei K.-J., Ubagai T., Polymeropoulos M.H., Moses S.W., Parvari R., Hershkovitz E., Mandel H., Fryman M., Chou J.Y. The gene for glycogen-storage disease type 1b maps to chromosome 11q23. Am. J. Hum. Genet. 1998;62:400–405. doi: 10.1086/301727. - DOI - PMC - PubMed
-
- Kishnani P.S., Austin S.L., Abdenur J.E., Arn P., Bali D.S., Boney A., Chung W.K., Dagli A.I., Dale D., Koeberl D., Somers M.J., Burns Wechsler S., Weinstein D.A., Wolfsdorf J.I., Watson M.S. Diagnosis and management of glycogen storage disease type I: a practice guideline of the American College of Medical Genetics and Genomics. Genet Med. 2014;16:e1. doi: 10.1038/gim.2014.128. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
