

doi: 10.1016/j.eats.2022.08.039.
eCollection 2022 Dec.
Arthroscopic Double-Row Repair of Posterosuperior Rotator Cuff Tears: Suture Bridge Technique Reinforced With Modified Mason-Allen and Simple Sutures
Affiliations
- PMID: 36632401
- PMCID: PMC9827121
- DOI: 10.1016/j.eats.2022.08.039
Item in Clipboard
Arthroscopic Double-Row Repair of Posterosuperior Rotator Cuff Tears: Suture Bridge Technique Reinforced With Modified Mason-Allen and Simple Sutures
Arthrosc Tech.
.
Abstract
Rotator cuff (RC) tears represent one of the most common causes of pain and dysfunction of the shoulder. Numerous RC repair techniques have been reported. In this Technical Note, we introduce an arthroscopic double-row repair technique that combines a suture bridge construct with modified Mason-Allen and simple suture fixation to optimize load-sharing and compression of the RC to the footprint. The described technique is ideal for crescent-shaped and large reparable U-shaped posterosuperior RC tears.
© 2022 The Authors.
Figures
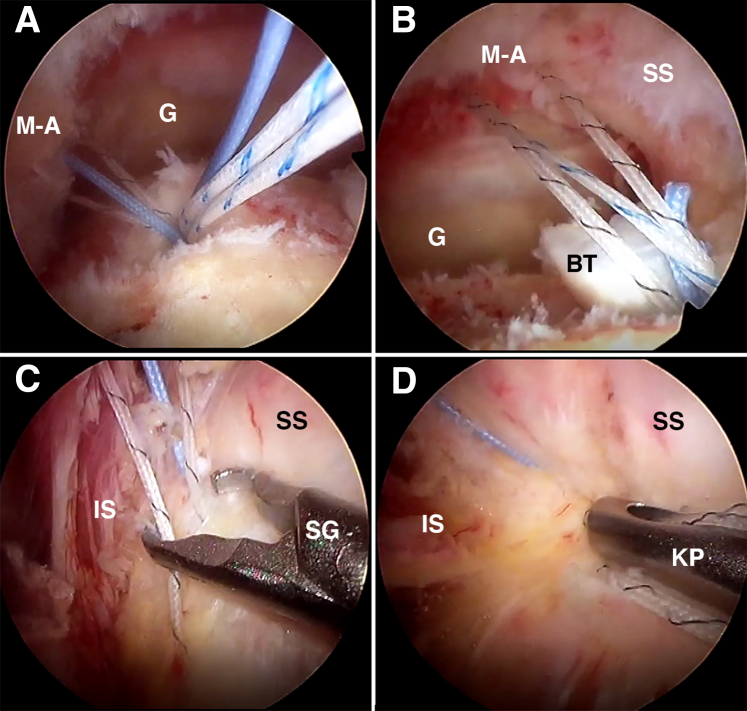
Arthroscopic visualization of the right shoulder (viewing from the lateral subacromial portal) with the patient in the beach-chair position reveals a large full-thickness, crescent-shaped tear of the supraspinatus (SS) and infraspinatus (IS) tendons. (A) Sutures from the posterior-medial anchor are passed from posterior-to-anterior in a modified Mason–Allen (M-A) configuration. (B) Sutures from the anterior-medial anchor are then passed in a similar fashion. Note, the long head biceps tendon (BT) has been tenodesed. (C and D) The 2 horizontal mattress sutures are then tied. (G, glenoid; KP, knot pusher; SG, suture grasper.)
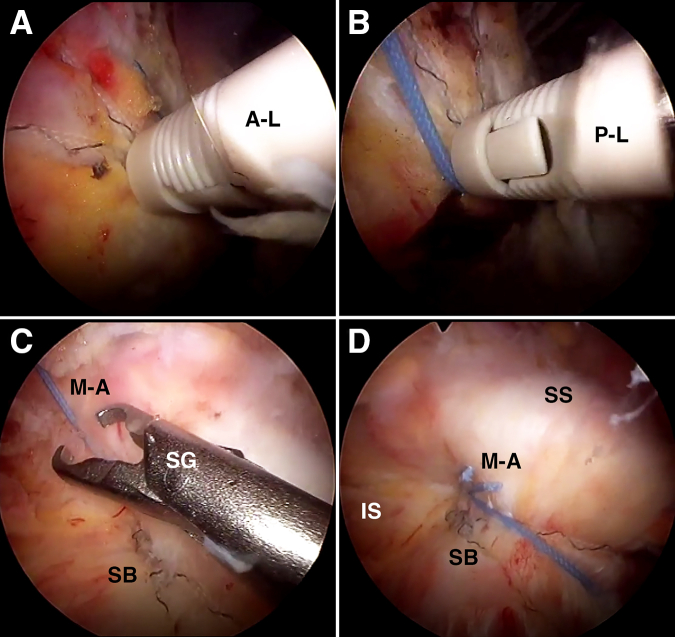
Arthroscopic visualization of the right shoulder (viewing from the lateral subacromial portal) with the patient in the beach-chair position. (A) In preparation for placement of the first lateral row anchor, one suture limb from each horizontal mattress suture and the free deep suture limb from the anterior-medial anchor that has not been shuttled through the supraspinatus tendon are loaded into a 4.5-mm knotless all-peek PopLok anchor (A-L, anterolateral anchor). (B) The process is repeated for placement of the second lateral row anchor within the posterolateral aspect of the greater tuberosity, in-line with the posterior-medial (P-M) anchor (P-L, posterolateral anchor). (C and D) The 2 appropriately paired suture limbs from the P-M and P-L anchors are then tied, reinforcing the suture bridge (SB) construct with a modified Mason-Allen suture (M-A); the process is repeated anteriorly. (IS, infraspinatus; SG, suture grasper; SS, supraspinatus.)
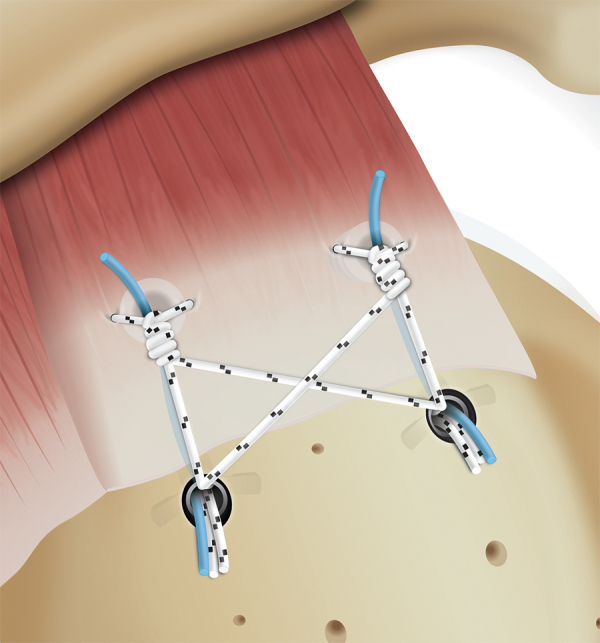
Illustration of a right shoulder (superior view) summarizing the steps required to complete the suture bridge portion of the rotator cuff repair.
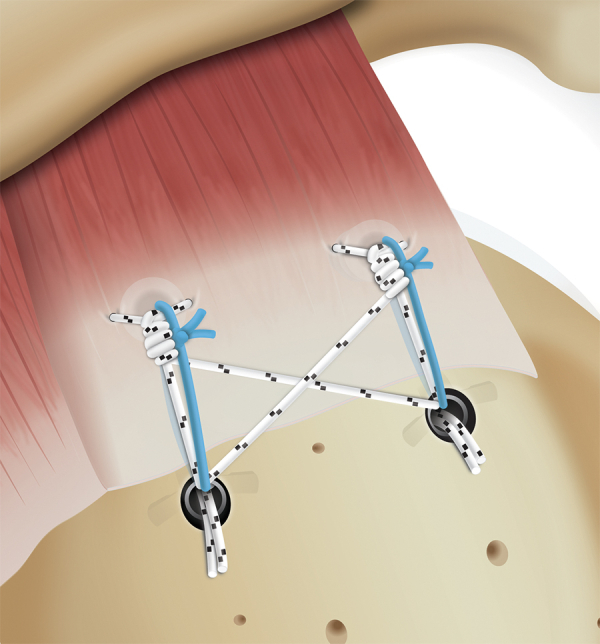
Illustration of a right shoulder (superior view). After completing the suture bridge portion of the rotator cuff repair, the 2 appropriately paired suture limbs from the posteromedial and posterolateral anchors are tied, reinforcing the suture bridge construct with a modified Mason–Allen suture. The process is repeated anteriorly.
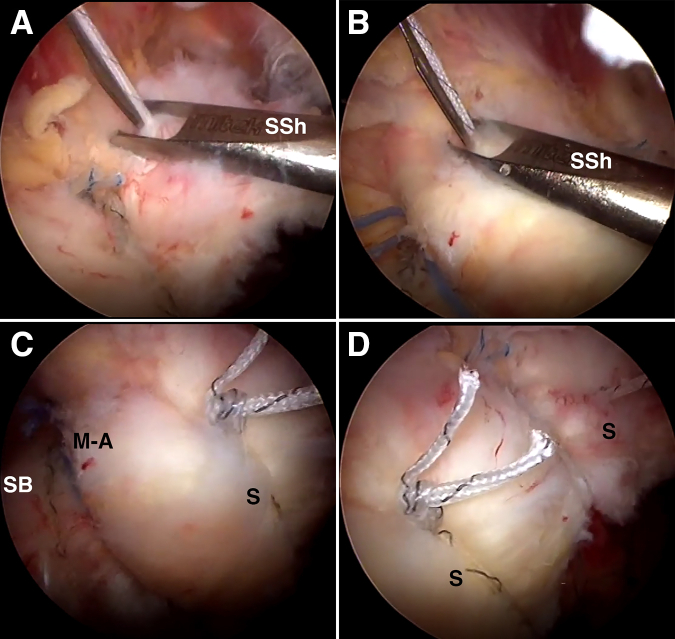
Arthroscopic visualization of the right shoulder (viewing from the lateral subacromial portal) with the patient in the beach chair position. (A) The anterolateral portal serves as the working portal to pass 1 of the 2 suture limbs captured and remaining within the anterolateral anchor through the anterior margin of the supraspinatus tendon in a simple fashion using an antegrade suture shuttle (SSh). (B) One of the 2 suture limbs remaining within the posterolateral anchor is used to address a remaining tendon gap/dog ear within the central aspect of the repaired rotator cuff. (C and D) The passed simple sutures (S) are then tied. (M-A, Mason–Allen; SB, suture bridge.)
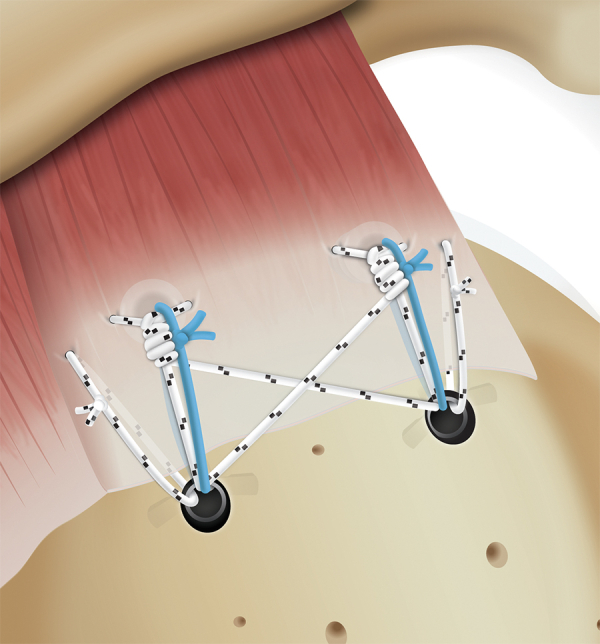
Illustration of a right shoulder (superior view) summarizing the final double-row rotator cuff repair construct. The suture bridge is reinforced with modified Mason–Allen sutures, which is then further secured with simple sutures passed along the free margin of the rotator cuff tendon to compress the tendon to the prepared footprint.
Similar articles
-
Clinical Outcomes of Modified Mason-Allen Single-Row Repair for Bursal-Sided Partial-Thickness Rotator Cuff Tears: Comparison With the Double-Row Suture-Bridge Technique.Am J Sports Med. 2015 Aug;43(8):1976-82. doi: 10.1177/0363546515587718. Epub 2015 Jun 8. Am J Sports Med. 2015. PMID: 26055919
-
Clinical outcomes and repair integrity after arthroscopic full-thickness rotator cuff repair: suture-bridge versus double-row modified Mason-Allen technique.J Shoulder Elbow Surg. 2018 Nov;27(11):1953-1959. doi: 10.1016/j.jse.2018.04.005. Epub 2018 May 24. J Shoulder Elbow Surg. 2018. PMID: 29803504
-
Arthroscopic modified Mason-Allen technique for large U- or L-shaped rotator cuff tears.Knee Surg Sports Traumatol Arthrosc. 2017 Jul;25(7):2129-2137. doi: 10.1007/s00167-016-4028-y. Epub 2016 Feb 5. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 26850514
-
[Massive tears of rotator cuff - comparison of mini-open and arthroscopic techniques. Part 1. Mini-open technique].Acta Chir Orthop Traumatol Cech. 2006 Dec;73(6):387-93. Acta Chir Orthop Traumatol Cech. 2006. PMID: 17266840 Czech.
-
Does Suture Technique Affect Re-Rupture in Arthroscopic Rotator Cuff Repair? A Meta-analysis.Arthroscopy. 2015 Aug;31(8):1576-82. doi: 10.1016/j.arthro.2015.02.004. Epub 2015 Mar 29. Arthroscopy. 2015. PMID: 25828166
Cited by
-
A Modified Mason-Allen Suture Enhancement Technique (Sunglasses Loop) for Single-Row Repair of Medium-to-Large Rotator Cuffs.Arthrosc Tech. 2024 May 10;13(7):103007. doi: 10.1016/j.eats.2024.103007. eCollection 2024 Jul. Arthrosc Tech. 2024. PMID: 39100258 Free PMC article.
-
A Narrative Review on the Double Pulley-Triple Row Technique for Large to Massive Rotator Cuff Repair.Clin Orthop Surg. 2025 Jun;17(3):359-371. doi: 10.4055/cios24424. Epub 2025 May 15. Clin Orthop Surg. 2025. PMID: 40454127 Free PMC article. Review.
-
Quantification and Predictors of Hemoglobin Drop, Hidden Blood Loss and Irrigation Fluid Retention in Shoulder Arthroscopy.J Clin Med. 2025 May 30;14(11):3875. doi: 10.3390/jcm14113875. J Clin Med. 2025. PMID: 40507637 Free PMC article.
References
-
- Park M.C., Elattrache N.S., Ahmad C.S., Tibone J.E. "Transosseous-equivalent" rotator cuff repair technique. Arthroscopy. 2006;22:1360.e1–1360.e5. - PubMed
-
- Shi B.Y., Diaz M., Binkley M., McFarland E.G., Srikumaran U. Biomechanical strength of rotator cuff repairs: A systematic review and meta-regression analysis of cadaveric studies. Am J Sports Med. 2018;47:1984–1993. - PubMed
-
- Gerber C., Schneeberger A.G., Perren S.M., Nyffeler R.W. Experimental rotator cuff repair. A preliminary study. J Bone Joint Surg Am. 1999;81:1281–1290. - PubMed
-
- Cho N.S., Yi J.W., Lee B.G., Rhee Y.G. Retear patterns after arthroscopic rotator cuff repair: Single-row versus suture bridge technique. Am J Sports Med. 2010;38:664–671. - PubMed
LinkOut - more resources
Full Text Sources
