

Arthroscopic Biologic Tuberoplasty for Irreparable Rotator Cuff Tears: An Expedited Technique
- PMID: 36632403
- PMCID: PMC9827058
- DOI: 10.1016/j.eats.2022.08.035
Arthroscopic Biologic Tuberoplasty for Irreparable Rotator Cuff Tears: An Expedited Technique
Abstract
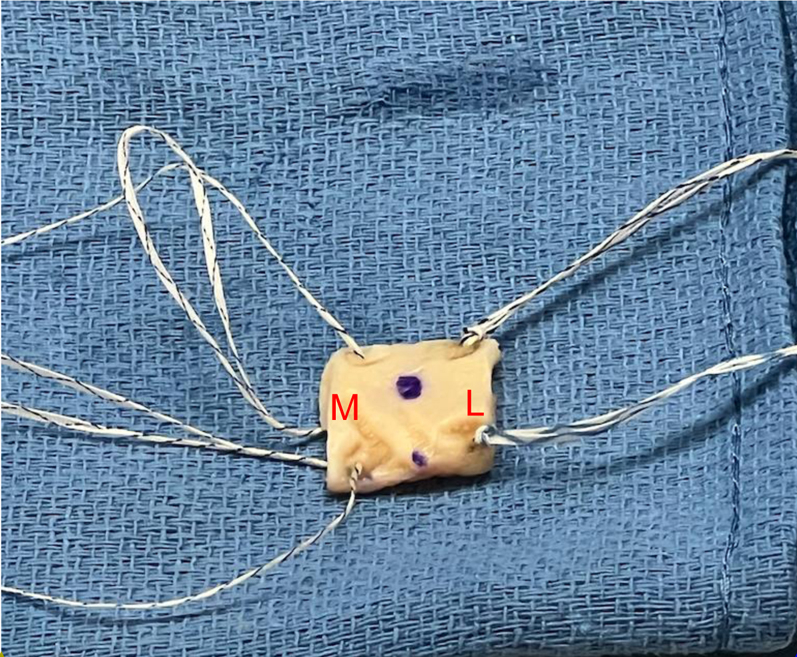
Massive irreparable rotator cuff tears in patients for whom arthroplasty is not an option can be a challenging clinical scenario for shoulder surgeons to manage. To achieve the best patient outcomes, a myriad of options has been presented in the literature, including debridement with biceps tenotomy or tenodesis, various tendon transfer procedures, superior capsular reconstruction, biceps tendon rerouting, bursal acromion resurfacing, balloon spacers, and tuberoplasty. While debridement with biceps tenotomy and superior capsular reconstruction have historically provided improvements in patient-reported outcomes, high rates of arthritis progression and failure of graft healing have been noted with these techniques, respectively. The superior capsular reconstruction has also proven to be technically challenging. The biologic tuberoplasty procedure was developed after several studies noted a lack of correlation between graft healing and improvement in patient-reported outcomes in superior capsular reconstructions, as long as the tuberosity remained covered with the graft. We present a technically efficient and expedited technique using an acellular human dermal allograft.
© 2022 The Authors.
Figures





References
-
- Neer C.S., 2nd, Craig E.V., Fukuda H. Cuff-tear arthropathy. J Bone Joint Surg Am. 1983;65:1232–1244. - PubMed
-
- Liem D., Lengers N., Dedy N., et al. Arthroscopic debridement of massive irreparable rotator cuff tears. Arthroscopy. 2008;24:743–748. - PubMed
-
- Walch G., Edwards T.B., Boulahia A., et al. Arthroscopic tenotomy of the long head of the biceps in the treatment of rotator cuff tears: clinical and radiographic results of 307 cases. J Shoulder Elbow Surg. 2005;14:238–246. - PubMed
-
- Elhassan B.T., Sanchez-Sotelo J., Wagner E.R. Outcome of arthroscopically assisted lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tears. J Shoulder Elbow Surg. 2020;29:2135–2142. - PubMed
-
- Gerber C., Rahm S.A., Catanzaro S., Farshad M., Moor B.K. Latissimus dorsi tendon transfer for treatment of irreparable posterosuperior rotator cuff tears: Long-term results at a minimum follow-up of ten years. J Bone Joint Surg Am. 2013;95:1920–1926. - PubMed
LinkOut - more resources
Full Text Sources
