

Elevated Uric Acid Is Associated With New-Onset Atrial Fibrillation: Results From the Swedish AMORIS Cohort
- PMID: 36633024
- PMCID: PMC9973652
- DOI: 10.1161/JAHA.122.027089
Elevated Uric Acid Is Associated With New-Onset Atrial Fibrillation: Results From the Swedish AMORIS Cohort
Abstract
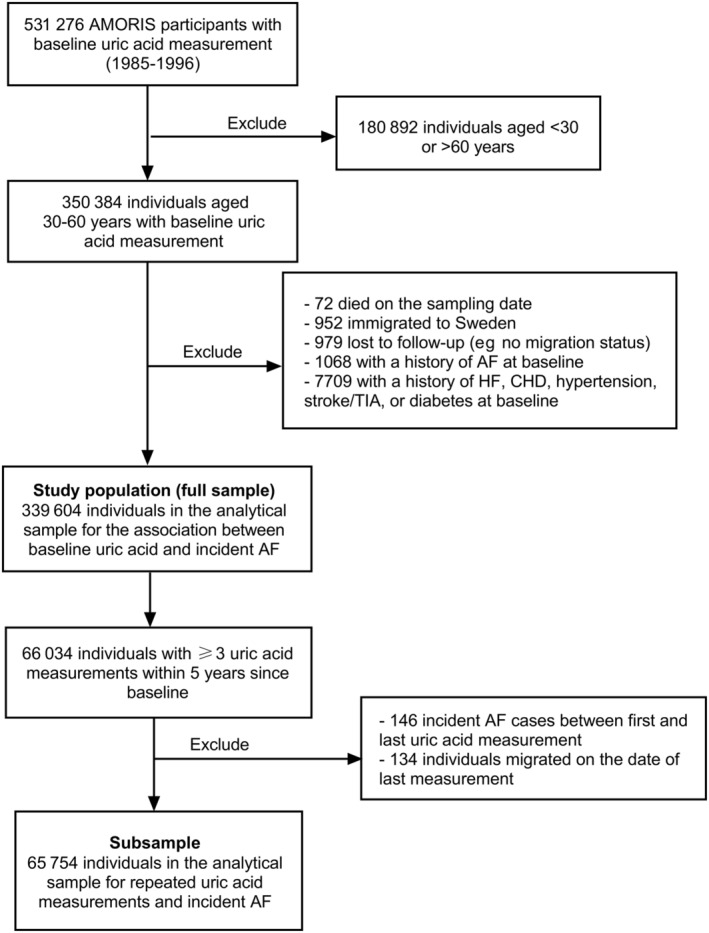
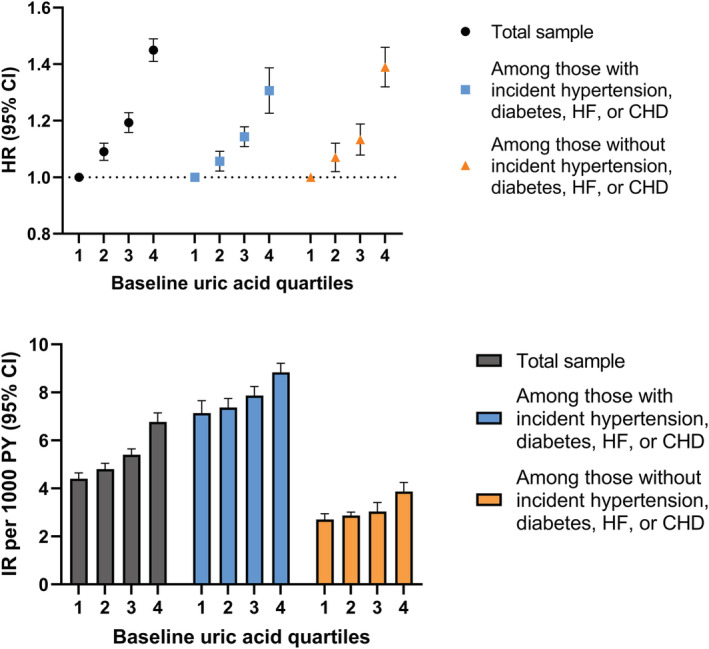
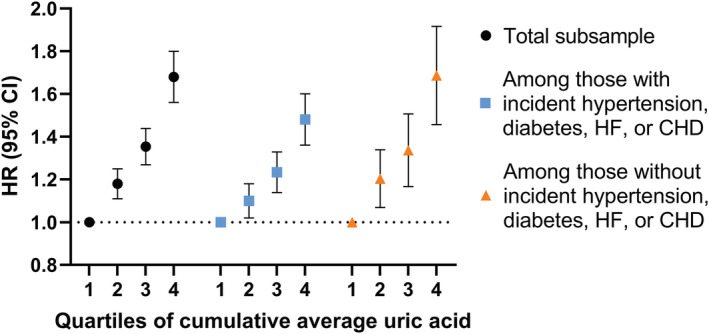
Background The role of uric acid is gaining increasing importance in the evaluation of cardiovascular disease, but its relationship with atrial fibrillation (AF) is unclear. This study aims to investigate the association between uric acid levels and risk of new-onset AF. Methods and Results A total of 339 604 individuals 30 to 60 years of age and free from cardiovascular disease at baseline (1985-1996) in the Swedish AMORIS (Apolipoprotein-Mortality Risk) cohort were followed until December 31, 2019 for incident AF. Cox regression models were used to examine the association between uric acid and AF, adjusting for potential confounders and stratifying by incident cardiovascular disease. Over a mean follow-up of 25.9 years, 46 516 incident AF cases occurred. Compared with the lowest uric acid quartile, each of the upper 3 quartiles were associated with an increased risk of AF in a dose-response manner. Adjusted hazard ratios were 1.09 (95% CI, 1.06-1.12) for second quartile, 1.19 (95% CI, 1.16-1.23) for third quartile, and 1.45 (95% CI, 1.41-1.49) for fourth quartile. The association was similar among individuals with and without incident hypertension, diabetes, heart failure, or coronary heart disease. The dose-response pattern was further supported in a subsample of individuals with repeated measurements of uric acid. Conclusions Elevated uric acid was associated with an increased risk of AF, not only among people with cardiovascular disease and cardiovascular risk factors but also among those without. Future investigations are needed to examine whether lowering uric acid is relevant for AF prevention.
Keywords: atrial fibrillation; biomarkers; cardiovascular disease; cohort studies; uric acid.
Figures
References
-
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton‐Cheh C, Lubitz SA, Magnani JW, Ellinor PT, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham heart study: a cohort study. Lancet. 2015;386:154–162. doi: 10.1016/S0140-6736(14)61774-8 - DOI - PMC - PubMed
-
- Allan V, Honarbakhsh S, Casas JP, Wallace J, Hunter R, Schilling R, Perel P, Morley K, Banerjee A, Hemingway H. Are cardiovascular risk factors also associated with the incidence of atrial fibrillation?: a systematic review and field synopsis of 23 factors in 32 population‐based cohorts of 20 million participants. Thromb Haemost. 2017;117:837–850. doi: 10.1160/TH16-11-0825 - DOI - PMC - PubMed
-
- Schnabel RB, Sullivan LM, Levy D, Pencina MJ, Massaro JM, D'Agostino RB, Newton‐Cheh C, Yamamoto JF, Magnani JW, Tadros TM, et al. Development of a risk score for atrial fibrillation (Framingham heart study): a community‐based cohort study. Lancet. 2009;373:739–745. doi: 10.1016/S0140-6736(09)60443-8 - DOI - PMC - PubMed
-
- Huxley RR, Lopez FL, Folsom AR, Agarwal SK, Loehr LR, Soliman EZ, MacLehose R, Konety S, Alonso A. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the atherosclerosis risk in communities (ARIC) study. Circulation. 2011;123:1501–1508. doi: 10.1161/CIRCULATIONAHA.110.009035 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
