

Colonisation with Extended-Spectrum Cephalosporin-Resistant Enterobacterales and Infection Risk in Surgical Patients: A Systematic Review and Meta-analysis
- PMID: 36633819
- PMCID: PMC9925622
- DOI: 10.1007/s40121-022-00756-z
Colonisation with Extended-Spectrum Cephalosporin-Resistant Enterobacterales and Infection Risk in Surgical Patients: A Systematic Review and Meta-analysis
Abstract
Introduction: Limited evidence has been reported for surgical site infections (SSIs) in patients undergoing surgery who are carriers of extended-spectrum cephalosporin-resistant Enterobacterales (ESCR-E). A systematic review and meta-analysis were conducted to evaluate the risk of postoperative infections in adult inpatients colonised with ESCR-E before surgery.
Methods: The Medline, Embase and Cochrane databases were searched between January 2011 and April 2022, following PRISMA indications. Random effects meta-analysis was used to quantify the association between ESCR-E colonisation and infection.
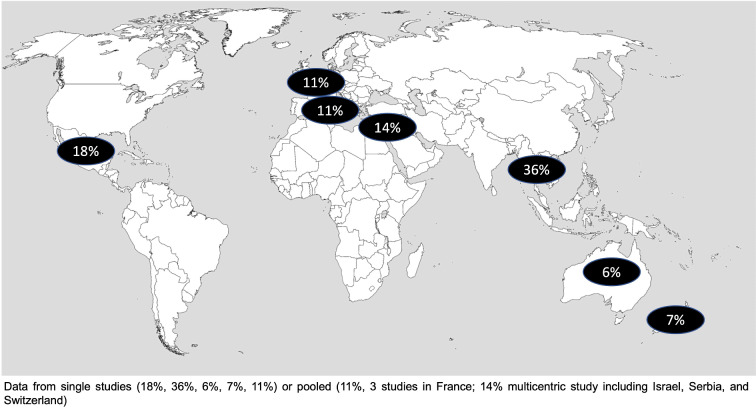
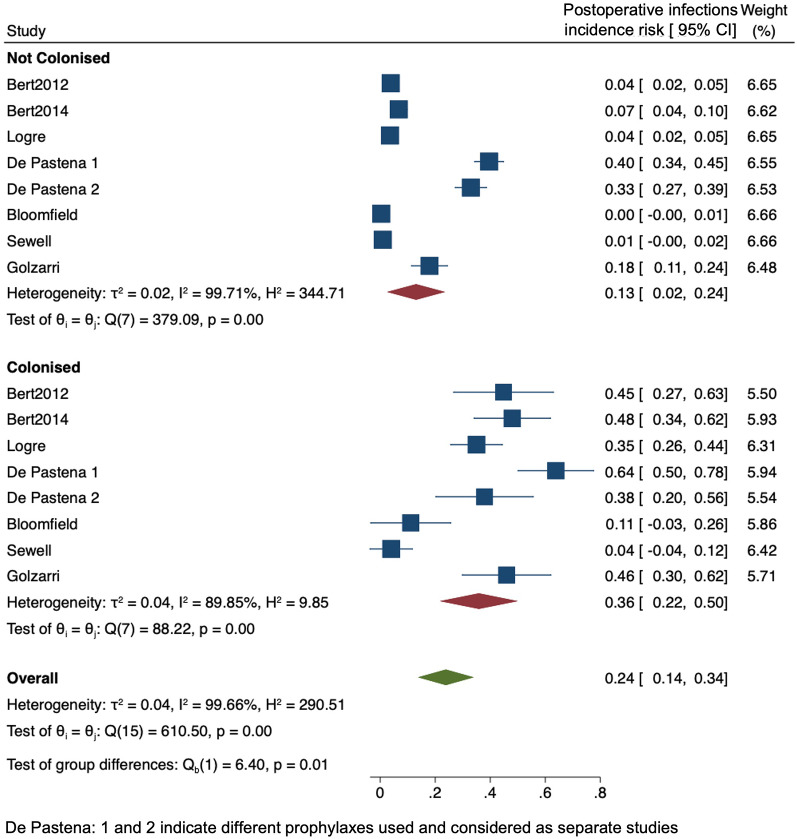
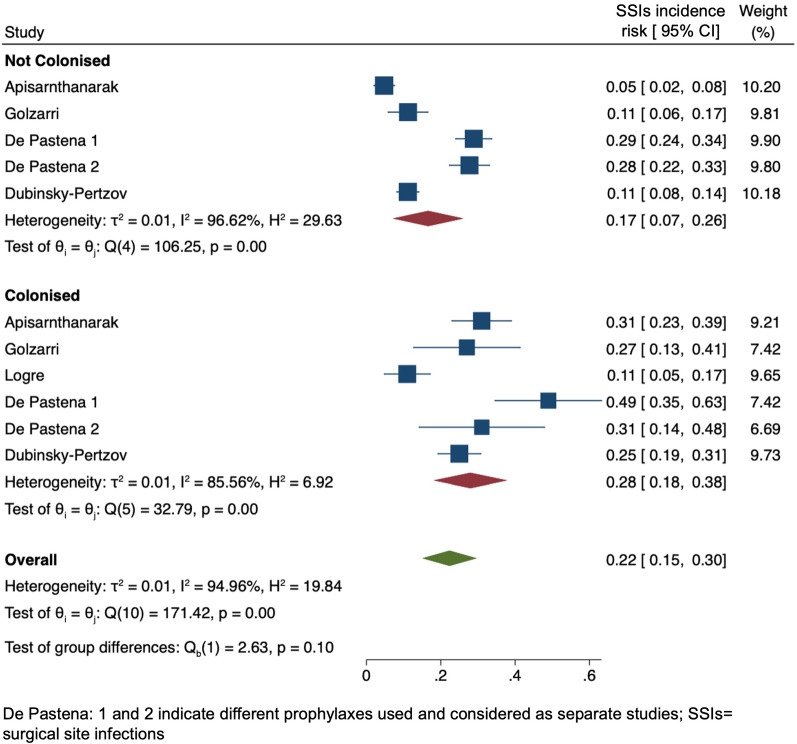
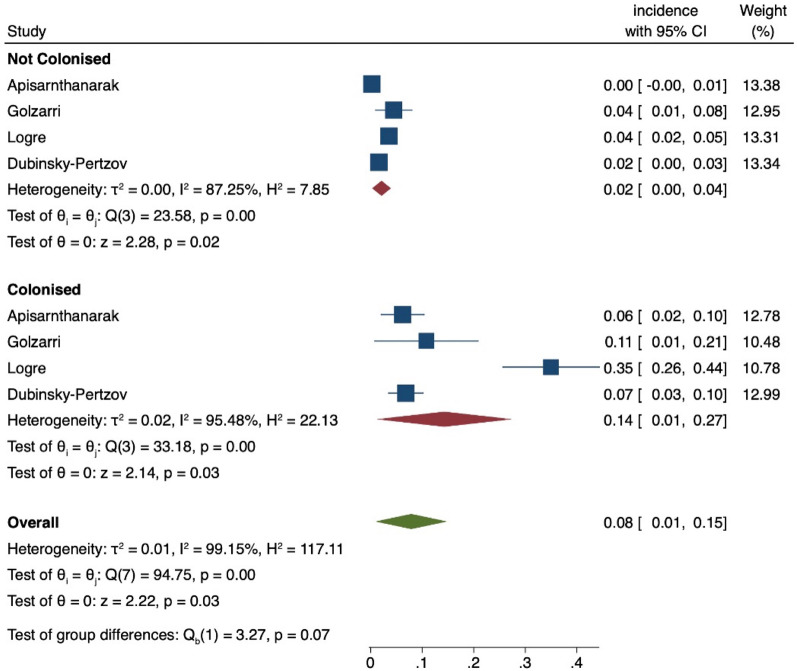
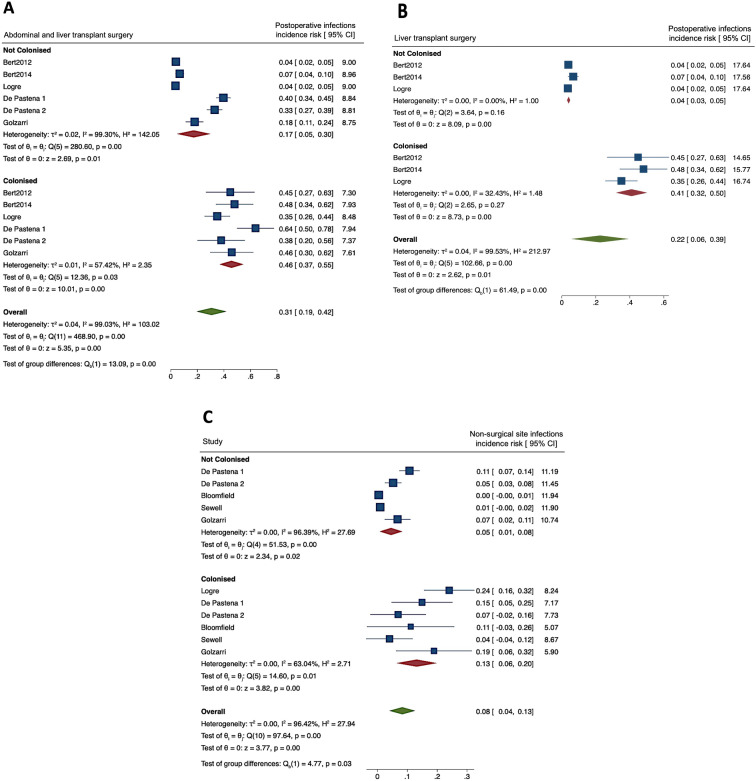
Results: Among the 467 articles reviewed, 9 observational studies encompassing 7219 adult patients undergoing surgery were included. The ESCR-E colonisation rate was 13.7% (95% CI 7.7-19.7). The most commonly reported surgeries included abdominal surgery (44%) and liver transplantation (LT; 33%). The SSI rate was 23.2% (95% CI 13.2-33.1). Pooled incidence risk was 0.36 (95% CI 0.22-0.50) vs 0.13 (95% CI 0.02-0.24) for any postoperative infection and 0.28 (95% CI 0.18-0.38) vs 0.17 (95% CI 0.07-0.26) for SSIs in ESCR-E carriers vs noncarriers, respectively. In ESCR-E carriers, the ESCR-E infection ratio was 7 times higher than noncarriers. Postoperative infection risk was higher in carriers versus noncarriers following LT. Sources of detected heterogeneity between studies included ESCR-E colonisation and the geographic region of origin.
Conclusions: Patients colonised with ESCR-E before surgery had increased incidence rates of post-surgical infections and SSIs compared to noncarriers. Our results suggest considering the implementation of pre-surgical screening for detecting ESCR-E colonisation status according to the type of surgery and the local epidemiology.
Keywords: Extended-spectrum cephalosporin-resistant Enterobacterales (ESCR-E); Meta-analysis; Postoperative infections; Rectal colonisation; Surgical site infections.
© 2023. The Author(s).
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
