

Individual variation in Plasmodium vivax malaria risk: Are repeatedly infected people just unlucky?
- PMID: 36634044
- PMCID: PMC9836309
- DOI: 10.1371/journal.pntd.0011020
Individual variation in Plasmodium vivax malaria risk: Are repeatedly infected people just unlucky?
Abstract
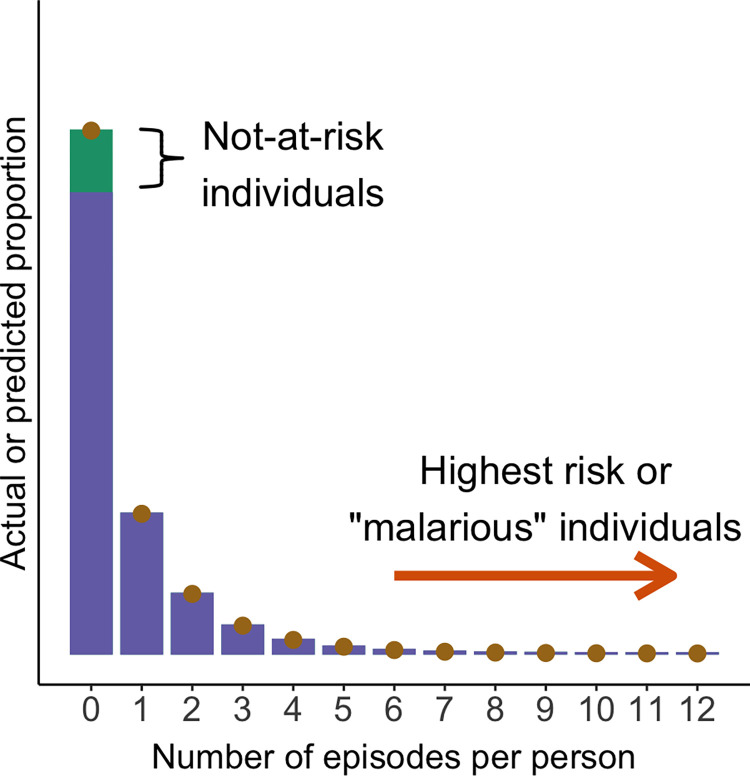
Extensive research has examined why some people have frequent Plasmodium falciparum malaria episodes in sub-Saharan Africa while others remain free of disease most of the time. In contrast, malaria risk heterogeneity remains little studied in regions where P. vivax is the dominant species. Are repeatedly infected people in vivax malaria settings such as the Amazon just unlucky? Here, we briefly review evidence that human genetic polymorphism and acquired immunity after repeated exposure to parasites can modulate the risk of P. vivax infection and disease in predictable ways. One-fifth of the hosts account for 80% or more of the community-wide vivax malaria burden and contribute disproportionally to onward transmission, representing a priority target of more intensive interventions to achieve malaria elimination. Importantly, high-risk individuals eventually develop clinical immunity, even in areas with very low or residual malaria transmission, and may constitute a large but silent parasite reservoir.
Copyright: © 2023 Corder et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- O’Meara WP, Simmons R, Bullins P, Freedman B, Abel L, Mangeni J, et al.. Mosquito exposure and malaria morbidity: a microlevel analysis of household mosquito populations and malaria in a population-based longitudinal cohort in Western Kenya. J Infect Dis. 2020;221:1176–1184. doi: 10.1093/infdis/jiz561 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
