

Potential long-term effects of SARS-CoV-2 infection on the pulmonary vasculature: Multilayered cross-talks in the setting of coinfections and comorbidities
- PMID: 36634048
- PMCID: PMC9836319
- DOI: 10.1371/journal.ppat.1011063
Potential long-term effects of SARS-CoV-2 infection on the pulmonary vasculature: Multilayered cross-talks in the setting of coinfections and comorbidities
Abstract
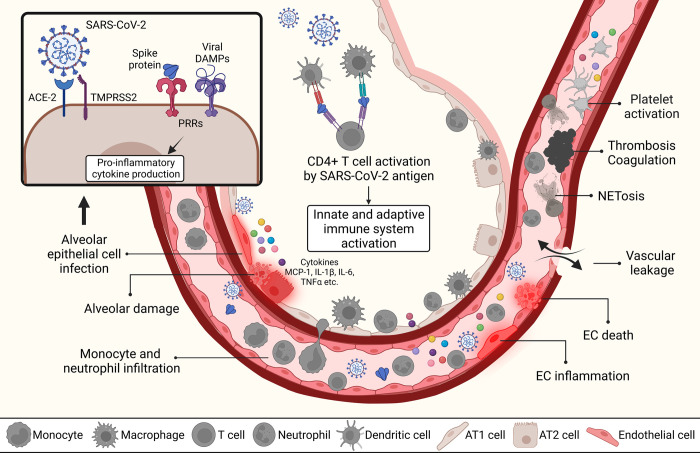
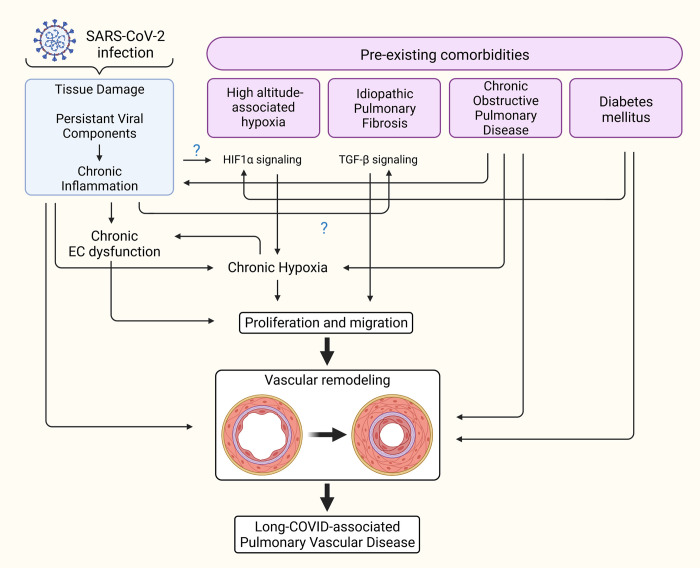
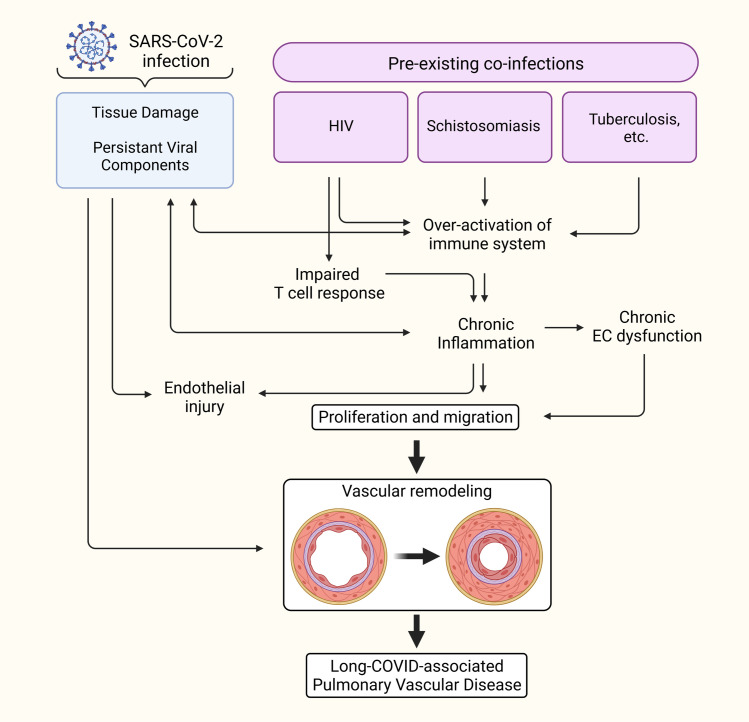
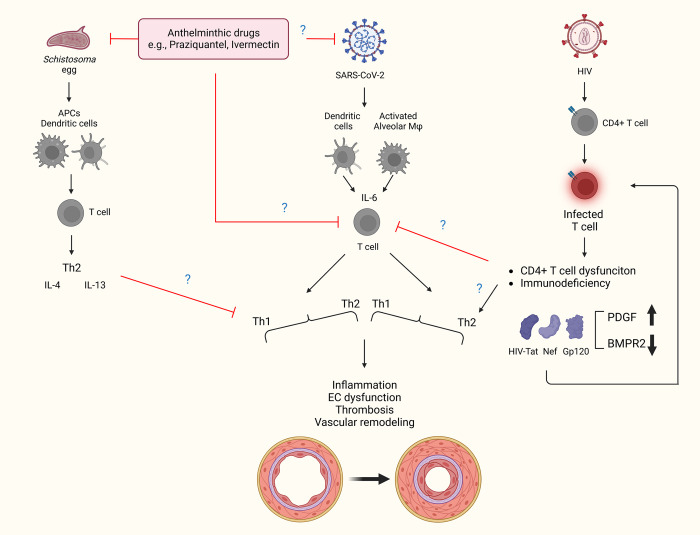
The Coronavirus Disease 2019 (COVID-19) caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and its sublineages pose a new challenge to healthcare systems worldwide due to its ability to efficiently spread in immunized populations and its resistance to currently available therapies. COVID-19, although targeting primarily the respiratory system, is also now well established that later affects every organ in the body. Most importantly, despite the available therapy and vaccine-elicited protection, the long-term consequences of viral infection in breakthrough and asymptomatic individuals are areas of concern. In the past two years, investigators accumulated evidence on how the virus triggers our immune system and the molecular signals involved in the cross-talk between immune cells and structural cells in the pulmonary vasculature to drive pathological lung complications such as endothelial dysfunction and thrombosis. In the review, we emphasize recent updates on the pathophysiological inflammatory and immune responses associated with SARS-CoV-2 infection and their potential long-term consequences that may consequently lead to the development of pulmonary vascular diseases.
Copyright: © 2023 Kumar et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
