

Sybil: A Validated Deep Learning Model to Predict Future Lung Cancer Risk From a Single Low-Dose Chest Computed Tomography
- PMID: 36634294
- PMCID: PMC10419602
- DOI: 10.1200/JCO.22.01345
Sybil: A Validated Deep Learning Model to Predict Future Lung Cancer Risk From a Single Low-Dose Chest Computed Tomography
Abstract
Purpose: Low-dose computed tomography (LDCT) for lung cancer screening is effective, although most eligible people are not being screened. Tools that provide personalized future cancer risk assessment could focus approaches toward those most likely to benefit. We hypothesized that a deep learning model assessing the entire volumetric LDCT data could be built to predict individual risk without requiring additional demographic or clinical data.
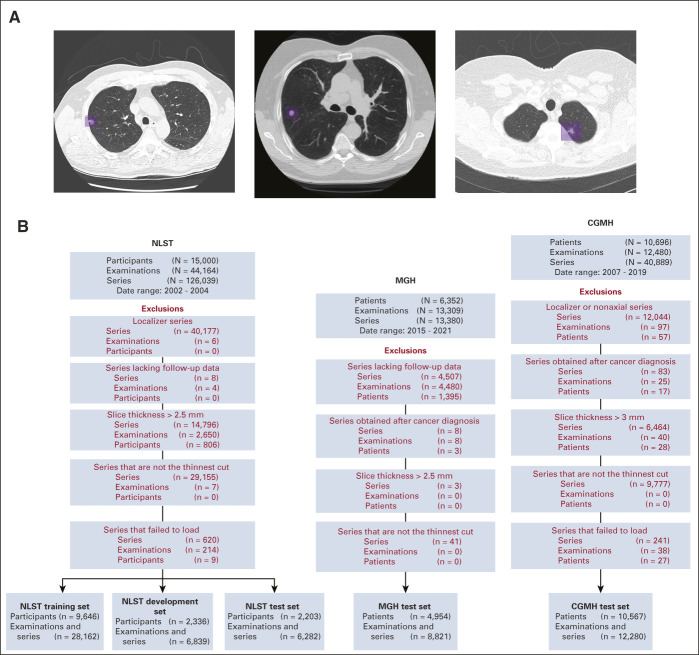
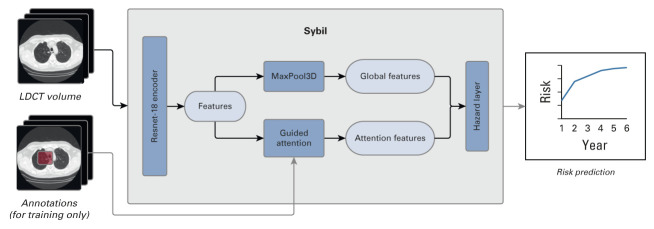
Methods: We developed a model called Sybil using LDCTs from the National Lung Screening Trial (NLST). Sybil requires only one LDCT and does not require clinical data or radiologist annotations; it can run in real time in the background on a radiology reading station. Sybil was validated on three independent data sets: a heldout set of 6,282 LDCTs from NLST participants, 8,821 LDCTs from Massachusetts General Hospital (MGH), and 12,280 LDCTs from Chang Gung Memorial Hospital (CGMH, which included people with a range of smoking history including nonsmokers).
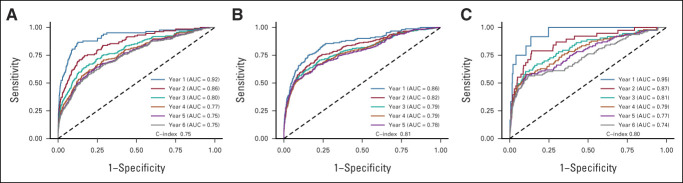
Results: Sybil achieved area under the receiver-operator curves for lung cancer prediction at 1 year of 0.92 (95% CI, 0.88 to 0.95) on NLST, 0.86 (95% CI, 0.82 to 0.90) on MGH, and 0.94 (95% CI, 0.91 to 1.00) on CGMH external validation sets. Concordance indices over 6 years were 0.75 (95% CI, 0.72 to 0.78), 0.81 (95% CI, 0.77 to 0.85), and 0.80 (95% CI, 0.75 to 0.86) for NLST, MGH, and CGMH, respectively.
Conclusion: Sybil can accurately predict an individual's future lung cancer risk from a single LDCT scan to further enable personalized screening. Future study is required to understand Sybil's clinical applications. Our model and annotations are publicly available.
[Media: see text].
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures
Comment in
-
Beyond the AJR: Should Imaging-Based Risk Assessment Tools Be Used in Lung Cancer Screening?AJR Am J Roentgenol. 2023 Sep;221(3):390. doi: 10.2214/AJR.23.29060. Epub 2023 Feb 1. AJR Am J Roentgenol. 2023. PMID: 36722762 Free PMC article. No abstract available.
-
The Intersection of Lung Cancer Screening, Radiomics, and Artificial Intelligence: Can One Scan Really Predict the Future Development of Lung Cancer?J Clin Oncol. 2023 Apr 20;41(12):2141-2143. doi: 10.1200/JCO.22.02885. Epub 2023 Feb 3. J Clin Oncol. 2023. PMID: 36735897 No abstract available.
-
Predicting Future Lung Cancer Risk from a Single Low-Dose CT Using Deep Learning.Radiol Imaging Cancer. 2023 May;5(3):e239013. doi: 10.1148/rycan.239013. Radiol Imaging Cancer. 2023. PMID: 37233206 Free PMC article. No abstract available.
-
Future lung cancer prediction using low-dose chest computed tomography.Transl Lung Cancer Res. 2023 Jul 31;12(7):1652-1654. doi: 10.21037/tlcr-23-235. Epub 2023 May 23. Transl Lung Cancer Res. 2023. PMID: 37577305 Free PMC article. No abstract available.
-
Role of Artificial Intelligence in Assisting Pulmonary and Critical Care Clinical Decision-Making.Am J Respir Crit Care Med. 2024 Sep 1;210(5):662-664. doi: 10.1164/rccm.202402-0331RR. Am J Respir Crit Care Med. 2024. PMID: 38924771 No abstract available.
References
-
- US Preventive Services Task Force, Krist AH Davidson KW et al. : Screening for lung cancer: US Preventive Services Task Force recommendation statement. JAMA 325:962-970, 2021 - PubMed
-
- Wang GX, Baggett TP, Pandharipande PV, et al. : Barriers to lung cancer screening engagement from the patient and provider perspective. Radiology 290:278-287, 2019 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
