

Anti-Integrin αvβ6 Autoantibodies Are a Novel Biomarker That Antedate Ulcerative Colitis
- PMID: 36634824
- PMCID: PMC10284061
- DOI: 10.1053/j.gastro.2022.12.042
Anti-Integrin αvβ6 Autoantibodies Are a Novel Biomarker That Antedate Ulcerative Colitis
Abstract
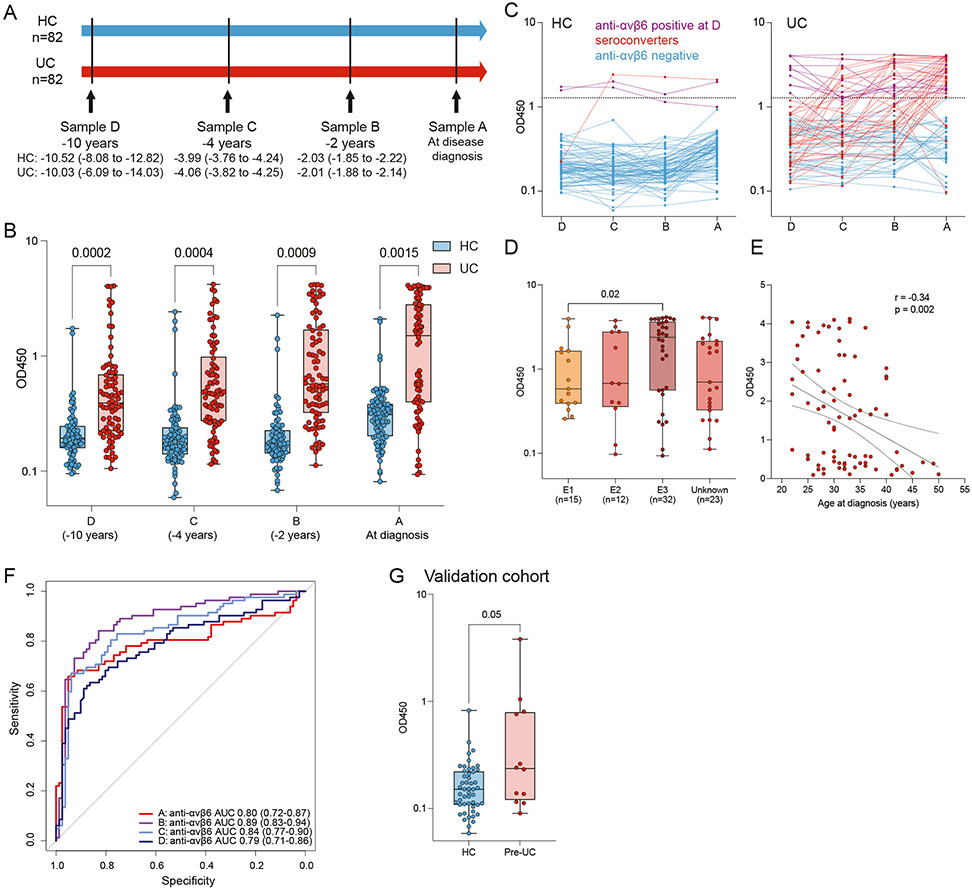
Background & aims: Better biomarkers for prediction of ulcerative colitis (UC) development and prognostication are needed. Anti-integrin αvβ6 (anti-αvβ6) autoantibodies have been described in patients with UC. We tested for the presence of anti-αvβ6 antibodies in the preclinical phase of UC and studied their association with disease-related outcomes after diagnosis.
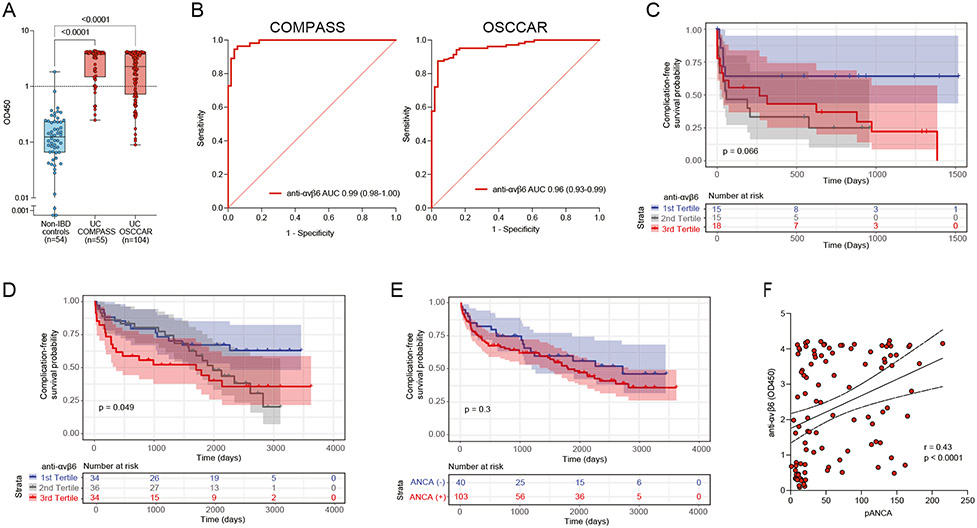
Methods: Anti-αvβ6 autoantibodies were measured in 4 longitudinal serum samples collected from 82 subjects who later developed UC and 82 matched controls from a Department of Defense preclinical cohort (PREDICTS [Proteomic Evaluation and Discovery in an IBD Cohort of Tri-service Subjects]). In a distinct, external validation cohort (Crohn's and Colitis Canada Genetic Environmental Microbial project cohort), we tested 12 pre-UC subjects and 49 matched controls. Furthermore, anti-αvβ6 autoantibodies were measured in 2 incident UC cohorts (COMPASS [Comprehensive Care for the Recently Diagnosed IBD Patients], n = 55 and OSCCAR [Ocean State Crohn's and Colitis Area Registry], n = 104) and associations between anti-αvβ6 autoantibodies and UC-related outcomes were defined using Cox proportional hazards model.
Results: Anti-αvβ6 autoantibodies were significantly higher among individuals who developed UC compared with controls up to 10 years before diagnosis in PREDICTS. The anti-αvβ6 autoantibody seropositivity was 12.2% 10 years before diagnosis and increased to 52.4% at the time of diagnosis in subjects who developed UC compared with 2.7% in controls across the 4 time points. Anti-αvβ6 autoantibodies predicted UC development with an area under the curve of at least 0.8 up to 10 years before diagnosis. The presence of anti-αvβ6 autoantibodies in preclinical UC samples was validated in the GEM cohort. Finally, high anti-αvβ6 autoantibodies was associated with a composite of adverse UC outcomes, including hospitalization, disease extension, colectomy, systemic steroid use, and/or escalation to biologic therapy in recently diagnosed UC.
Conclusions: Anti-integrin αvβ6 autoantibodies precede the clinical diagnosis of UC by up to 10 years and are associated with adverse UC-related outcomes.
Keywords: Anti-Integrin αvβ6; Autoantibodies; Biomarkers; Inflammatory Bowel Disease; Ulcerative Colitis.
Copyright © 2023 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
These authors disclose the following: Saurabh Mehandru reports receiving research grants from Genentech and Takeda; receiving payment for lectures from Takeda, Genentech, and Morphic; and receiving consulting fees from Takeda, Morphic, Ferring, and Arena Pharmaceuticals. Jean-Frederic Colombel reports receiving research grants from AbbVie, Janssen Pharmaceuticals, and Takeda; receiving payment for lectures from AbbVie, Amgen, Allergan, Inc. Ferring Pharmaceuticals, Shire, and Takeda; receiving consulting fees from AbbVie, Amgen, Arena Pharmaceuticals, Boehringer Ingelheim, BMS, Celgene Corporation, Eli Lilly, Ferring Pharmaceuticals, Galmed Research, Genentech, Glaxo Smith Kline, Janssen Pharmaceuticals, Kaleido Biosciences, Imedex, Immunic, Iterative Scopes, Merck, Microbia, Novartis, PBM Capital, Pfizer, Protagonist Therapeutics, Sanofi, Takeda, TiGenix, Vifor; and holds stock options in Intestinal Biotech Development. Ryan C. Ungaro has served as an advisory board member or consultant for AbbVie, Bristol Myer Squibb, Janssen, Pfizer, and Takeda; research support from AbbVie, Boehringer Ingelheim, Eli Lily, and Pfizer. Thierry Dervieux is an employee of Prometheus Laboratories and hold stock options. Joseph A. Murray reports receiving grants from Nexpep/ImmusanT, National Institutes of Health, Immunogenix, Takeda Pharmaceutical, Allakos, Oberkotter, Cour; and consultancy fees from Bionix, Lilly Research Laboratory, Johnson & Johnson, Dr. Schar USA, UCB Biopharma, Celimmune, Intrexon Corporation, Dren Bio, Reistone pharma, Chugai Pharma, Kanyos, Boehringer Ingelheim, Equillium, and Torax Medical. Sacha Gnjatic reports other research funding from Genentech, Boehringer-Ingelheim, EMD Serono, Takeda, and Regeneron. Joana Torres received grants from AbbVie and Janssen, payment for lectures from Janssen, AbbVie, and Pfizer, and consulting fees from Janssen, AbbVie, Pfizer, and BMS. Dean Sheppard is a founder of Pliant Therapeutics, receives research funding from AbbVie, and is on the Scientific Review Board for Genentech and Amgen. The remaining authors disclose no conflicts.
Figures
References
-
- Bonen DK, Cho JH. The genetics of inflammatory bowel disease. Gastroenterology 2003;124:521–536. - PubMed
-
- NIDDK IBD Genetics Consortium Phenotype Operating Manual. Published May 10, 2006. Accessed February 1, 2023. https://repository.niddk.nih.gov/media/studies/ibd/ibd_phenotyping-manua....
-
- Torres J, Petralia F, Sato T, et al. Serum biomarkers identify patients who will develop inflammatory bowel diseases up to 5 years before diagnosis. Gastroenterology 2020;159:96–104. - PubMed
-
- Lee SH, Turpin W, Espin-Garcia O, et al. Anti-microbial antibody response is associated with future onset of Crohn’s disease independent of biomarkers of altered gut barrier function, subclinical inflammation, and genetic risk. Gastroenterology 2021;161:1540–1551. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
