

Improved benefit of continuing luspatercept therapy: sub-analysis of patients with lower-risk MDS in the MEDALIST study
- PMID: 36635381
- PMCID: PMC9889415
- DOI: 10.1007/s00277-022-05071-8
Improved benefit of continuing luspatercept therapy: sub-analysis of patients with lower-risk MDS in the MEDALIST study
Abstract
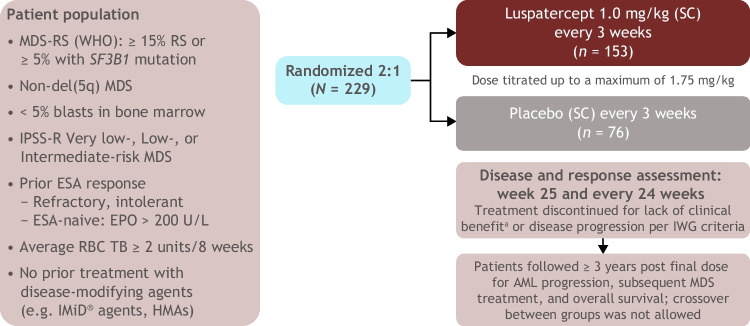
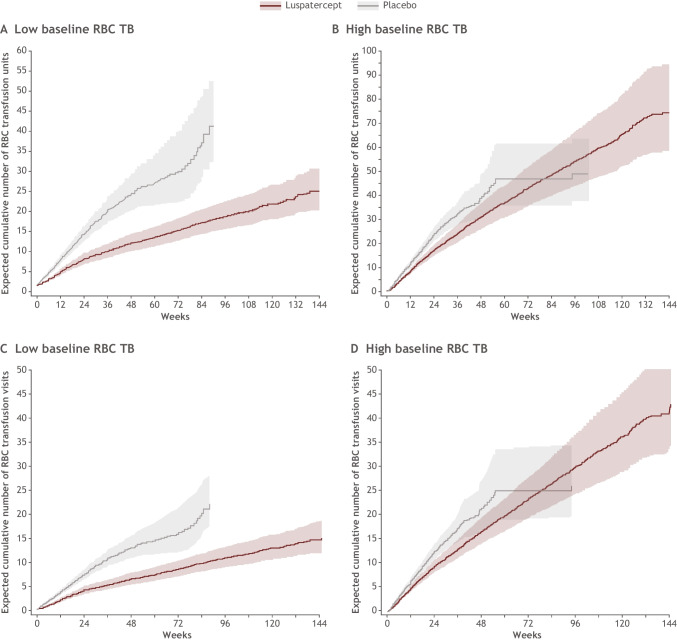
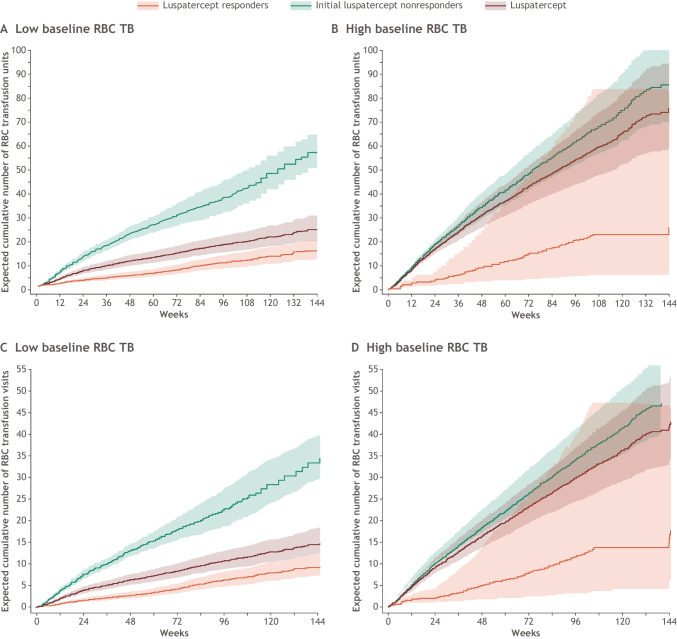
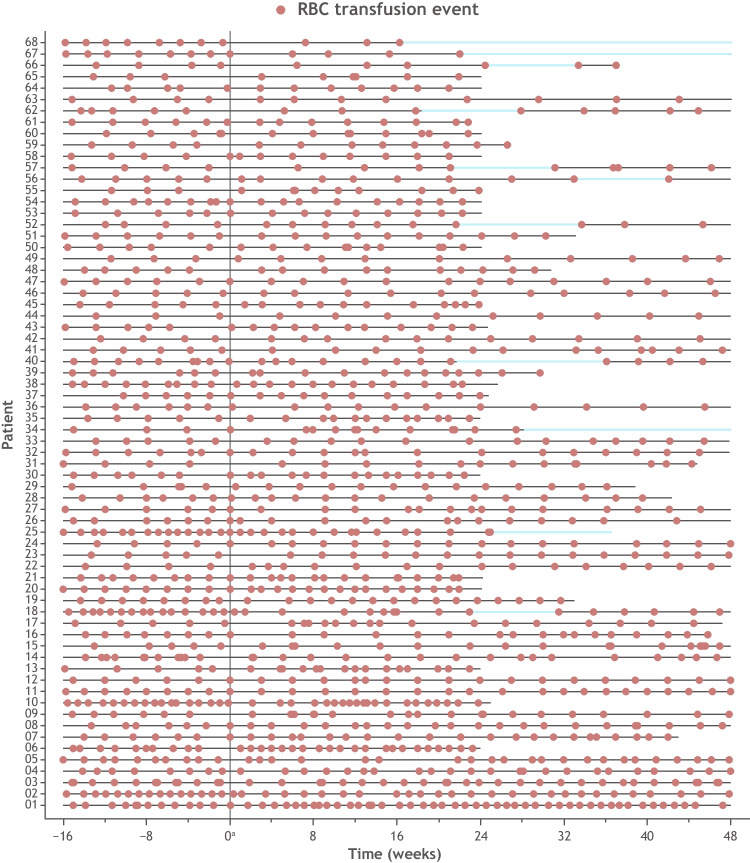
Red blood cell transfusion independence (RBC-TI) is an important goal in treating lower-risk myelodysplastic syndromes with ring sideroblasts. In the phase 3 MEDALIST study, RBC-TI of ≥ 8 weeks was achieved by significantly more luspatercept- versus placebo-treated patients in the first 24 weeks of treatment. In this post hoc analysis, we evaluated RBC transfusion units and visits based on patients' baseline transfusion burden level and the clinical benefit of luspatercept treatment beyond week 25 in initial luspatercept nonresponders (patients who did not achieve RBC-TI ≥ 8 weeks by week 25) but continued luspatercept up to 144 weeks. RBC transfusion burden, erythroid response, serum ferritin levels, and hemoglobin levels relative to baseline were evaluated. Through week 25, fewer RBC transfusion units and visits were observed in luspatercept-treated patients versus placebo, regardless of baseline transfusion burden. This continued through 144 weeks of luspatercept treatment, particularly in patients with low baseline transfusion burden. Sixty-eight patients were initial nonresponders at week 25 but continued treatment; most (81%) received the maximum dose of luspatercept (1.75 mg/kg). Sixteen percent achieved RBC-TI for ≥ 8 weeks during weeks 25-48, 26% had reduced RBC transfusion burden, 10% achieved an erythroid response, 44% had reduced serum ferritin, and hemoglobin levels increased an average of 1.3 g/dL from baseline. These data have implications for clinical practice, as transfusion units and visits are less in luspatercept-treated patients through week 25 regardless of baseline transfusion burden, and continuing luspatercept beyond week 25 can potentially provide additional clinical benefits for initial nonresponders. Trial registration: NCT02631070.
Keywords: Anemia; Health-related quality of life; Luspatercept; Myelodysplastic syndromes; Red blood cell transfusion independence.
© 2023. The Author(s).
Conflict of interest statement
UG has received research support from BMS and Novartis; speaker honorarium from BMS, Jazz Pharmaceuticals, and Novartis; and consulting fees from BMS. PF has received research support and honoraria from BMS. UP has received research funding from Amgen, BMS, Janssen, Merck, and Novartis; consulting fees from BMS; honoraria from AbbVie, BMS, Geron, Janssen, Novartis, and Takeda. RB has received research funding and honoraria for advisory boards from BMS and Taiho Pharma. VS has served on advisory boards for BMS, Geron, Gilead, Menarini, Novartis, and Takeda; and has served on speaker’s bureau for BMS and Novartis. MD-C reports honoraria, consulting fees, and travel support, and has served on advisory boards for BMS, Novartis, and Takeda. AY, DT, GZ, DM, and CH are employees of BMS, and hold stock ownership. SF and XH are employees of BMS. RZ is an employee of GSK and former employee of BMS. RSK reports consulting fees from AbbVie, Acceleron Pharma, BMS, Geron, Jazz Pharmaceuticals, and Novartis; and speakers bureau or honoraria for AbbVie, BMS, CTI BioPharma, Innovent, Jazz Pharmaceuticals, Novartis, PharmaEssentia, Taiho Oncology, and Takeda. AMZ reports consultancy fees from AbbVie, Acceleron, Agios, Amgen, Aprea, Astellas, BeyondSpring, Boehringer-Ingelheim, Cardiff Oncology, Cardinal Health, Celgene/BMS, Daiichi Sankyo, Epizyme, Geron, Gilead, Incyte, Ionis, Janssen, Jazz, Kura, Novartis, Otsuka, Pfizer, Seattle Genetics, Syndax, Taiho, Takeda, Trovagene, and Tyme; research funding for AbbVie, ADC Therapeutics, Amgen, Aprea, Astex, Boehringer-Ingelheim, Cardiff Oncology, BMS, Incyte, Medimmune/Astrazeneca, Novartis, Otsuka, Pfizer, Takeda, and Trovagene; honoraria for AbbVie, Acceleron, Agios, Amgen, Aprea, Astellas, Beyondpspring, Boehringer-Ingelheim, Cardiff Oncology, Cardinal Health, Celgene/BMS, Daiichi Sankyo, Epizyme, Geron, Gilead, Incyte, Ionis, Janssen, Jazz, Kura, Novartis, Otsuka, Pfizer, Seattle Genetics, Syndax, Taiho, Takeda, Trovagene, and Tyme; clinical trial committees for Abbvie, BMS, Geron, Gilead, Kura, and Novartis; and travel support for Cardiff Oncology, Novartis, and Pfizer. GG-M reports grant or research support from AbbVie, Amphivena, Aprea, BMS, Curis, Forty Seven, H3 Biomedicine, Helsinn, Merck, Novartis, and Onconova; and consultancy fees from Astex, BMS, Genentech, and Helsinn.
Figures


References
-
- Greenberg PL, Tuechler H, Schanz J, Sanz G, Garcia-Manero G, Solé F, Bennett JM, Bowen D, Fenaux P, Dreyfus F, Kantarjian H, Kuendgen A, Levis A, Malcovati L, Cazzola M, Cermak J, Fonatsch C, Le Beau MM, Slovak ML, Krieger O, Luebbert M, Maciejewski J, Magalhaes SM, Miyazaki Y, Pfeilstöcker M, Sekeres M, Sperr WR, Stauder R, Tauro S, Valent P, Vallespi T, van de Loosdrecht AA, Germing U, Haase D. Revised international prognostic scoring system for myelodysplastic syndromes. Blood. 2012;120:2454–2465. doi: 10.1182/blood-2012-03-420489. - DOI - PMC - PubMed
-
- Pfeilstöcker M, Tuechler H, Sanz G, Schanz J, Garcia-Manero G, Solé F, Bennett JM, Bowen D, Fenaux P, Dreyfus F, Kantarjian H, Kuendgen A, Malcovati L, Cazzola M, Cermak J, Fonatsch C, Le Beau MM, Slovak ML, Levis A, Luebbert M, Maciejewski J, Machherndl-Spandl S, Magalhaes SM, Miyazaki Y, Sekeres MA, Sperr WR, Stauder R, Tauro S, Valent P, Vallespi T, van de Loosdrecht AA, Germing U, Haase D, Greenberg PL. Time-dependent changes in mortality and transformation risk in MDS. Blood. 2016;128:902–910. doi: 10.1182/blood-2016-02-700054. - DOI - PMC - PubMed
-
- Neukirchen J, Lauseker M, Blum S, Giagounidis A, Lübbert M, Martino S, Siragusa S, Schlenk RF, Platzbecker U, Hofmann WK, Götze K, Palumbo GA, Magrin S, Kündgen A, Aul C, Hildebrandt B, Hasford J, Kobbe G, Haas R, Germing U. Validation of the revised international prognostic scoring system (IPSS-R) in patients with myelodysplastic syndrome: a multicenter study. Leuk Res. 2014;38:57–64. doi: 10.1016/j.leukres.2013.10.013. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
