

A machine learning framework develops a DNA replication stress model for predicting clinical outcomes and therapeutic vulnerability in primary prostate cancer
- PMID: 36635710
- PMCID: PMC9835390
- DOI: 10.1186/s12967-023-03872-7
A machine learning framework develops a DNA replication stress model for predicting clinical outcomes and therapeutic vulnerability in primary prostate cancer
Abstract
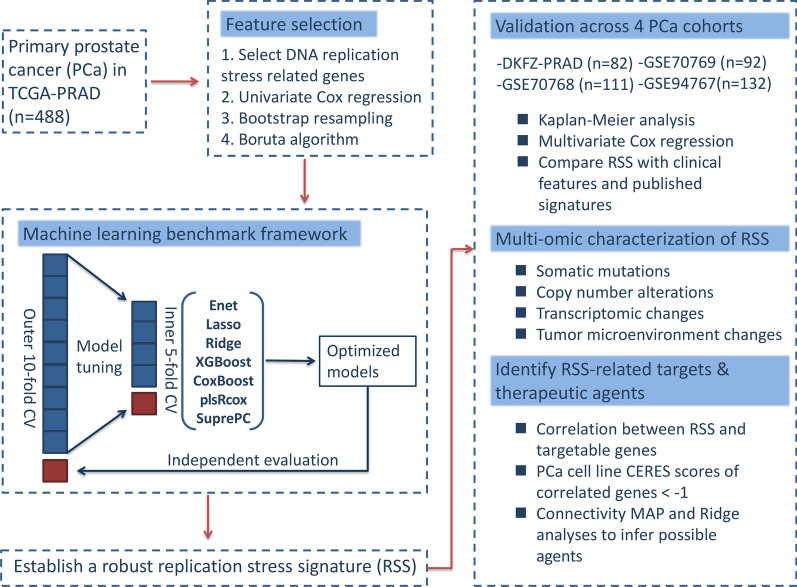
Recent studies have identified DNA replication stress as an important feature of advanced prostate cancer (PCa). The identification of biomarkers for DNA replication stress could therefore facilitate risk stratification and help inform treatment options for PCa. Here, we designed a robust machine learning-based framework to comprehensively explore the impact of DNA replication stress on prognosis and treatment in 5 PCa bulk transcriptomic cohorts with a total of 905 patients. Bootstrap resampling-based univariate Cox regression and Boruta algorithm were applied to select a subset of DNA replication stress genes that were more clinically relevant. Next, we benchmarked 7 survival-related machine-learning algorithms for PCa recurrence using nested cross-validation. Multi-omic and drug sensitivity data were also utilized to characterize PCa with various DNA replication stress. We found that the hyperparameter-tuned eXtreme Gradient Boosting model outperformed other tuned models and was therefore used to establish a robust replication stress signature (RSS). RSS demonstrated superior performance over most clinical features and other PCa signatures in predicting PCa recurrence across cohorts. Lower RSS was characterized by enriched metabolism pathways, high androgen activity, and a favorable prognosis. In contrast, higher RSS was significantly associated with TP53, RB1, and PTEN deletion, exhibited increased proliferation and DNA replication stress, and was more immune-suppressive with a higher chance of immunotherapy response. In silico screening identified 13 potential targets (e.g. TOP2A, CDK9, and RRM2) from 2249 druggable targets, and 2 therapeutic agents (irinotecan and topotecan) for RSS-high patients. Additionally, RSS-high patients were more responsive to taxane-based chemotherapy and Poly (ADP-ribose) polymerase inhibitors, whereas RSS-low patients were more sensitive to androgen deprivation therapy. In conclusion, a robust machine-learning framework was used to reveal the great potential of RSS for personalized risk stratification and therapeutic implications in PCa.
Keywords: DNA replication stress; Machine learning; Precision oncology; Prostate cancer.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures







Similar articles
-
Integrative multi-omics analysis unveils stemness-associated molecular subtypes in prostate cancer and pan-cancer: prognostic and therapeutic significance.J Transl Med. 2023 Nov 7;21(1):789. doi: 10.1186/s12967-023-04683-6. J Transl Med. 2023. PMID: 37936202 Free PMC article.
-
Integrated machine learning identifies epithelial cell marker genes for improving outcomes and immunotherapy in prostate cancer.J Transl Med. 2023 Nov 4;21(1):782. doi: 10.1186/s12967-023-04633-2. J Transl Med. 2023. PMID: 37925432 Free PMC article.
-
The established chemokine-related prognostic gene signature in prostate cancer: Implications for anti-androgen and immunotherapies.Front Immunol. 2022 Oct 6;13:1009634. doi: 10.3389/fimmu.2022.1009634. eCollection 2022. Front Immunol. 2022. PMID: 36275733 Free PMC article.
-
Androgen action in the prostate gland.Minerva Urol Nefrol. 2012 Mar;64(1):35-49. Minerva Urol Nefrol. 2012. PMID: 22402316 Review.
-
DNA-Damage-Repair Gene Alterations in Genitourinary Malignancies.Eur Surg Res. 2022;63(4):155-164. doi: 10.1159/000526415. Epub 2022 Aug 9. Eur Surg Res. 2022. PMID: 35944490 Review.
Cited by
-
Omics-Mediated Treatment for Advanced Prostate Cancer: Moving Towards Precision Oncology.Int J Mol Sci. 2025 Aug 2;26(15):7475. doi: 10.3390/ijms26157475. Int J Mol Sci. 2025. PMID: 40806607 Free PMC article. Review.
-
A DNA Replication Stress-Based Prognostic Model for Lung Adenocarcinoma.Acta Naturae. 2023 Jul-Sep;15(3):100-110. doi: 10.32607/actanaturae.25112. Acta Naturae. 2023. PMID: 37908773 Free PMC article.
-
Radiomics based on multiple machine learning methods for diagnosing early bone metastases not visible on CT images.Skeletal Radiol. 2025 Feb;54(2):335-343. doi: 10.1007/s00256-024-04752-x. Epub 2024 Jul 19. Skeletal Radiol. 2025. PMID: 39028463
-
The Potential Biological Roles and Clinical Significance of Anaphase-Promoting Complex Subunit 1 in Colorectal Cancer.Cancer Control. 2025 Jan-Dec;32:10732748251330059. doi: 10.1177/10732748251330059. Epub 2025 Apr 14. Cancer Control. 2025. PMID: 40229946 Free PMC article.
-
Leveraging a neutrophil-derived PCD signature to predict and stratify patients with acute myocardial infarction: from AI prediction to biological interpretation.J Transl Med. 2024 Jul 2;22(1):612. doi: 10.1186/s12967-024-05415-0. J Transl Med. 2024. PMID: 38956669 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
