

"THE MANTLE" bundle for minimizing cerebral hypoxia in severe traumatic brain injury
- PMID: 36635711
- PMCID: PMC9835224
- DOI: 10.1186/s13054-022-04242-3
"THE MANTLE" bundle for minimizing cerebral hypoxia in severe traumatic brain injury
Abstract
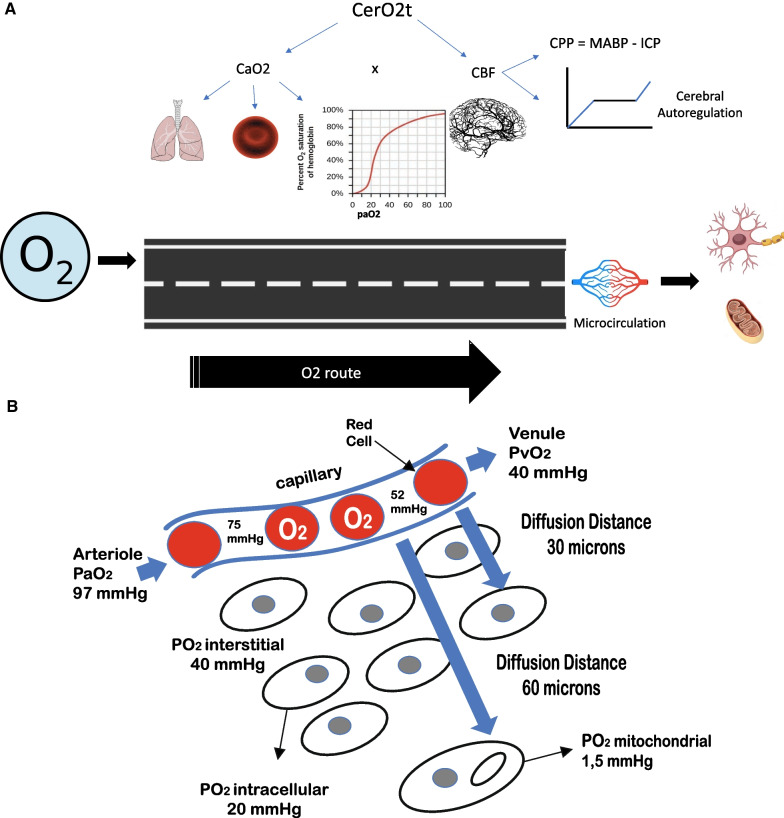
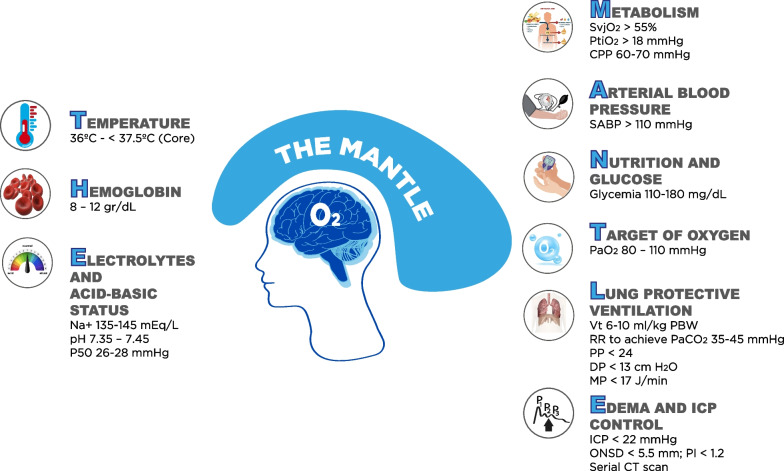
To ensure neuronal survival after severe traumatic brain injury, oxygen supply is essential. Cerebral tissue oxygenation represents the balance between oxygen supply and consumption, largely reflecting the adequacy of cerebral perfusion. Multiple physiological parameters determine the oxygen delivered to the brain, including blood pressure, hemoglobin level, systemic oxygenation, microcirculation and many factors are involved in the delivery of oxygen to its final recipient, through the respiratory chain. Brain tissue hypoxia occurs when the supply of oxygen is not adequate or when for some reasons it cannot be used at the cellular level. The causes of hypoxia are variable and can be analyzed pathophysiologically following "the oxygen route." The current trend is precision medicine, individualized and therapeutically directed to the pathophysiology of specific brain damage; however, this requires the availability of multimodal monitoring. For this purpose, we developed the acronym "THE MANTLE," a bundle of therapeutical interventions, which covers and protects the brain, optimizing the components of the oxygen transport system from ambient air to the mitochondria.
Keywords: Brain hypoxia; Brain oxygenation; Cerebral ischemia; Cerebral oxygenation monitoring; Traumatic brain injury.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Zauner A, Daugherty WP, Bullock MR, et al. Brain oxygenation and energy metabolism: part I-biological function and pathophysiology. Neurosurgery. 2002;51:289–301. - PubMed
-
- Marín-Caballos AJ, Murillo-Cabezas F, Domínguez-Roldan JM, Leal-Noval SR, Rincón-Ferrari MD, Muñoz-Sánchez MÁ. Monitorización de la presión tisular de oxígeno (PtiO2) en la hipoxia cerebral: aproximación diagnóstica y terapéutica. Med Intensiva. 2008;32(2):81–90. doi: 10.1016/S0210-5691(08)70912-4. - DOI - PubMed
-
- Oddo M, Levine JM, Mackenzie L, Frangos S, Feihl F, Kasner SE, Katsnelson M, Pukenas B, Macmurtrie E, Maloney-Wilensky E, Kofke WA, LeRoux PD. Brain hypoxia is associated with short-term outcome after severe traumatic brain injury independently of intracranial hypertension and low cerebral perfusion pressure. Neurosurgery. 2011;69(5):1037–45. doi: 10.1227/NEU.0b013e3182287ca7. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
