

Elevated Serum Fibroblast Growth Factor 23 (FGF-23) Perseveres into a Convalescence Period After Elective Cardiac Surgery, with Receptor Activator of Nuclear Factor κB Ligand (RANKL) and Cartilage Oligomeric Matrix Protein (COMP) Being Part of the Peri-Surgical -Pro-Arteriosclerotic Inflammatory Response
- PMID: 36635948
- PMCID: PMC9847201
- DOI: 10.12659/MSM.937934
Elevated Serum Fibroblast Growth Factor 23 (FGF-23) Perseveres into a Convalescence Period After Elective Cardiac Surgery, with Receptor Activator of Nuclear Factor κB Ligand (RANKL) and Cartilage Oligomeric Matrix Protein (COMP) Being Part of the Peri-Surgical -Pro-Arteriosclerotic Inflammatory Response
Abstract
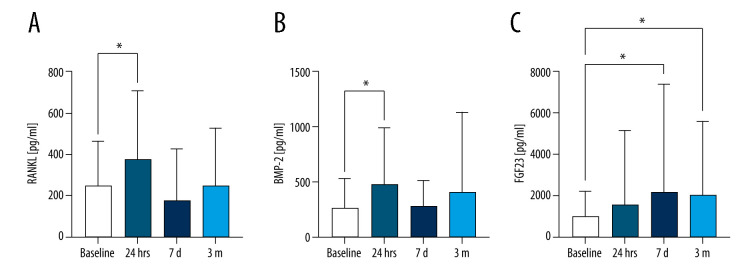
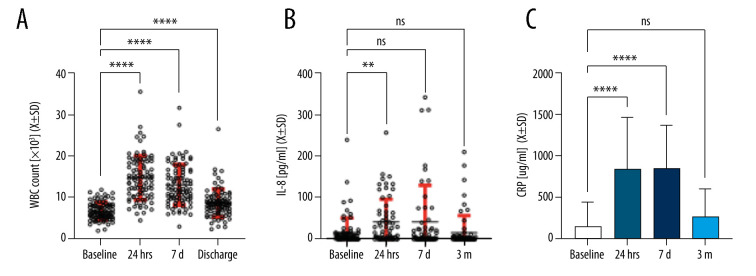
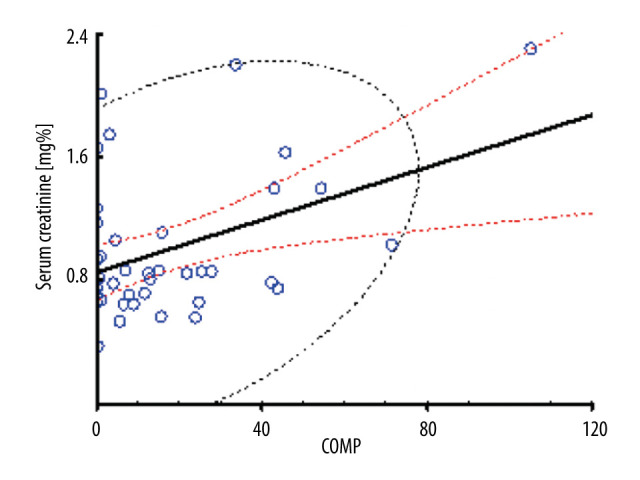
BACKGROUND Receptor activator of nuclear factor kappa B ligand (RANKL), osteoprotegerin (OPG), cartilage oligomeric matrix protein (COMP), bone morphogenetic protein (BMP-2), and fibroblast growth factor 23 (FGF-23) are involved in inflammation, calcium deposition, and fibrosis of blood vessels. Acute changes in these factors may contribute to the progression of arteriosclerosis, especially if their elevated serum levels persist postoperatively. MATERIAL AND METHODS A total of 90 patients (79 White, 4 African American, and 7 Other) undergoing elective heart surgery were enrolled in the study. Blood was collected before surgery and after surgery at 24 hours, 7 days, and 3 months to allow for longitudinal comparisons. After the plasma isolation, several biomarkers levels were studied using an enzymatic-linked assay. Demographic and clinical information were obtained from electronic health records. RESULTS At 24 hours after surgery, RANKL (RANKLbaseline=248.7±215.7 vs RANKLt24h=376.4±329.7; P=0.035), and BMP-2 (BMP-2baseline=283.7±255.4 vs BMP-2t24h=482.4; P=0.015) were significantly elevated compared to baseline, with levels returning to baseline at 7 days. FGF-23 increased significantly from baseline (FGF-23baseline=1020±1210) to 7 days (FGF-237d=2191±5188; P=0.029) and remained significantly higher than baseline at 3 months (FGF-233m=2041±3521; P=0.044). White blood cells (WBC) remained elevated at discharge (WBCbaseline=6.8±2.1 vs WBC24h=15.0±5.3 vs WBCdischarge=8.8±3.4). IL-8 and C-reactive protein normalized at 3 months. Estimated blood loss was significantly correlated with RANKL at 24 hours (r²=0.33; P=0.035). Serum creatinine levels after surgery at 24 hours (r²=0.41; p=0.008) and 7 days (r²=0.59; P=0.000) was strongly correlated with COMP. CONCLUSIONS Persistent elevation of serum FGF-23 indicates a potential for accelerated arteriosclerosis after cardiac surgery.
Conflict of interest statement
Figures
References
-
- Giacinto O, Satriano U, Nenna A, et al. Inflammatory response and endothelial dysfunction following cardiopulmonary bypass: Pathophysiology and pharmacological targets. Recent Pat Inflamm Allergy Drug Discov. 2019;13:158–73. - PubMed
-
- Mach L, Bedanova H, Soucek M, et al. Impact of cardiopulmonary bypass surgery on cytokines in epicardial adipose tissue: Comparison with subcutaneous fat. Perfusion. 2017;32:279–84. - PubMed
-
- McGuinness J, Bouchier-Hayes D, Redmond JM. Understanding the inflammatory response to cardiac surgery. Surgeon. 2008;6:162–71. - PubMed
-
- de Vries MR, Simons KH, Jukema JW, et al. Vein graft failure: From pathophysiology to clinical outcomes. Nat Rev Cardiol. 2016;13:451–70. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
