

A phase II trial of GSK2256098 and trametinib in patients with advanced pancreatic ductal adenocarcinoma
- PMID: 36636049
- PMCID: PMC9830369
- DOI: 10.21037/jgo-22-86
A phase II trial of GSK2256098 and trametinib in patients with advanced pancreatic ductal adenocarcinoma
Abstract
Background: Mitogen-activated protein kinase kinase (MEK) is activated by mutated KRAS in >90% of pancreatic ductal adenocarcinoma (PDAC). MEK and focal adhesion kinase (FAK) are frequently co-activated in PDAC providing a rationale for combining trametinib, an oral allosteric MEK1/2 inhibitor, with GSK2256098, an oral FAK inhibitor.
Methods: Advanced PDAC patients whose disease progressed after first line palliative chemotherapy were treated with GSK2256098 250 mg twice daily and trametinib 0.5 mg once daily orally. The primary endpoint was clinical benefit (CB; complete response, partial response, or stable disease ≥24 weeks). Twenty-four patients were planned to enroll using a 2-stage minimax design (P0=0.15, P1=0.40; alpha =0.05, power 0.86). The combination would be considered inactive if 2/12 or fewer patients achieved CB at the end of stage 1, and would be considered active if >7/24 response-evaluable patients achieved CB by the end of stage 2. Serial blood samples were collected for circulating tumor DNA (ctDNA) mutation profiling.
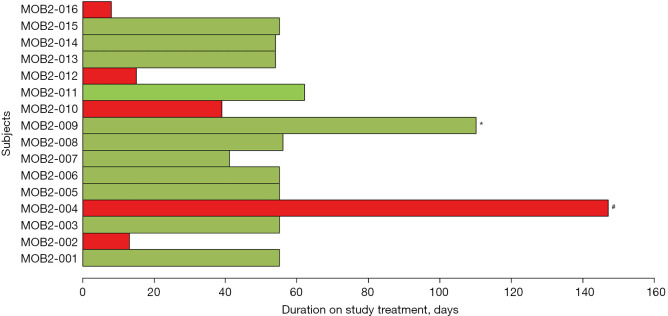
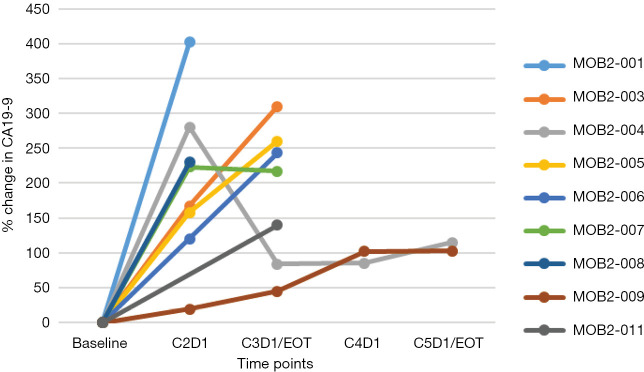
Results: Sixteen patients were enrolled and 11 were response evaluable. Of those 11, 10 had progressive disease as best tumor response and one had stable disease for 4 months. No treatment related grade ≥3 adverse events (AEs) were observed. The median progression free survival (PFS) was 1.6 (95% CI: 1.5-1.8) months and the median overall survival (OS) was 3.6 (95% CI: 2.7-not reached) months. One response-inevaluable patient achieved clinical stability for 5 months with reduction in CA19-9 and ctDNA levels with a MAP2K1 treatment resistance mutation detected in ctDNA at clinical progression.
Conclusions: The combination of GSK2256098 and trametinib was well tolerated but was not active in unselected advanced PDAC.
Keywords: FAK inhibition; GSK2256098; MEK inhibition; Pancreatic adenocarcinoma (PDAC); trametinib.
2022 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-22-86/coif). EM received honoraria from Novartis for advisory board and educational activities in melanoma. SW received consulting fees from Amgen and Seattle Genetics and honoraria from GSK, Merk, Eisai, and Pfizer for speaking engagements and participation in advisory boards (these engagements did not relate to pancreatic cancer, nor did they involve the agents studied in this clinical trial). LLS has consulting/advisory arrangements with Merck, Pfizer, Celgene, AstraZeneca, Morphosys, Roche, Oncorus, Symphogen, Seattle Genetics, GlaxoSmithKline, Voronoi, Arvinas, Tessa, Navire, Relay, Rubius, Janpix, Daiichi Sanyko; stock ownership of Agios (spouse); leadership position in Treadwell Therapeutics (spouse); and institution receives clinical trials support from Novartis, Bristol-Myers Squibb, Pfizer, Boerhinger-Ingelheim, GlaxoSmithKline, Roche/Genentech, Karyopharm, AstraZeneca, Merck, Celgene, Astellas, Bayer, Abbvie, Amgen, Symphogen, Intensity Therapeutics, Mirati Therapeutics, Shattucks, Avid; data safety monitor board participation with Mirati Therpeutics. PLB has uncompensated consulting/advisory arrangements with Merck, Lilly, BMS, SeaGen, Gilead, Amgen, Genentech/Roche; institution receives clinical trials support from Novartis, Bristol-Myers Squibb, Pfizer, GlaxoSmithKline, Roche/Genentech, AstraZeneca, Merck, Amgen, Sanofi, Nektar Therapeutics, Bicara Therapeutics, Sanofi, Lilly; data safety monitor board participation with Lilly. The other authors have no conflicts of interest to declare.
Figures

References
-
- Wang-Gillam A, Li CP, Bodoky G, et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, arvard ed, open-label, phase 3 trial. Lancet 2016;387:545-57. 10.1016/S0140-6736(15)00986-1 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous