

Rectal tumor fragmentation as a response pattern following chemoradiation
- PMID: 36636056
- PMCID: PMC9830359
- DOI: 10.21037/jgo-22-477
Rectal tumor fragmentation as a response pattern following chemoradiation
Abstract
Background: Tumor response to neoadjuvant therapy is heterogenous and prognostically important for locally advanced rectal adenocarcinoma (LARC) patients. Commonly applied response classification approaches including tumor regression grading (TRG) and TN downstaging can be discordant. The aim of this study is to compare the prognostic value of discordant tumor response measurement categorized according to the AJCC/CAP TRG schema and ypTN stage.
Methods: This is a single-center retrospective review of 90 consecutive patients with stage II-III rectal cancer receiving neoadjuvant chemoradiation (nCRT), total mesorectal excision (TME) and adjuvant chemotherapy (ACT) between 2007 and 2018. Two pathologists re-examined each case to assign a consensus AJCC TRG. A Cox proportional hazards ratio model assessed the effect of patient, tumor, and treatment factors on disease-free survival (DFS).
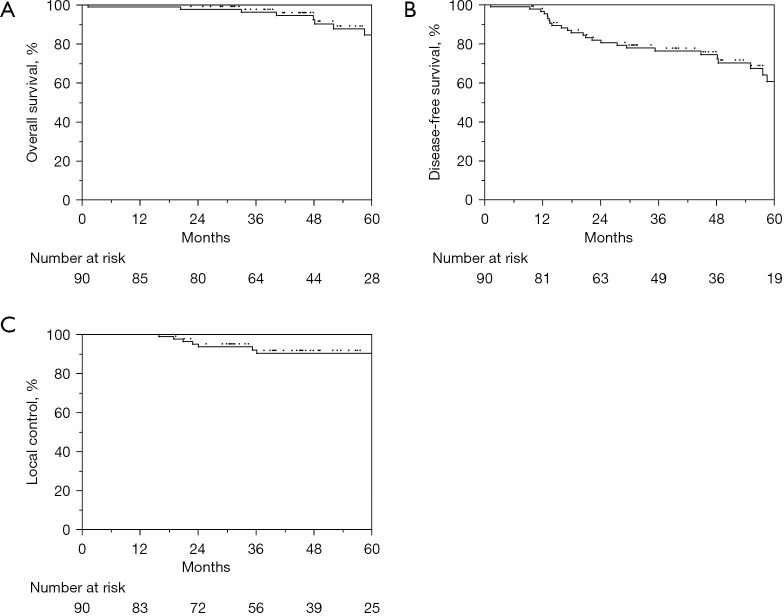
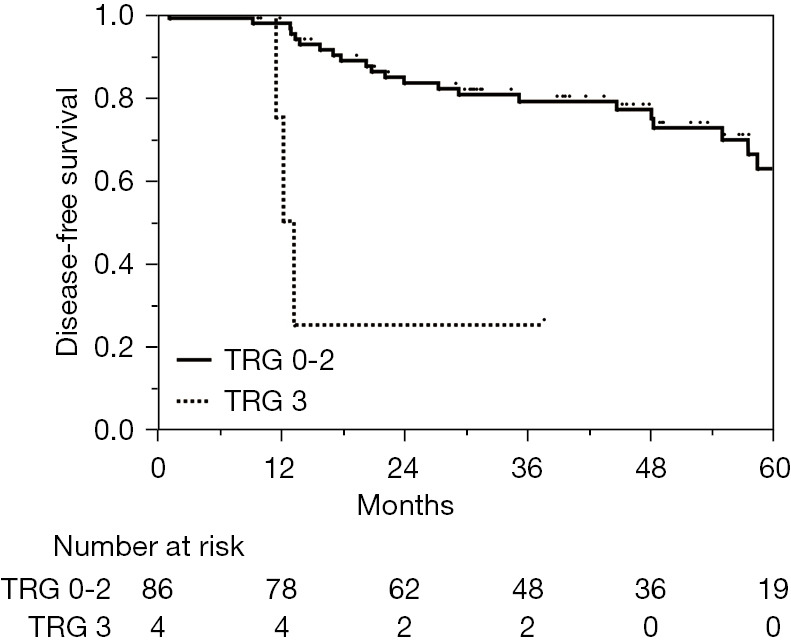
Results: Median follow-up after surgery was 46 months (95% CI: 41-50 months). Median age at diagnosis was 55 years (range: 27-80). Most patients were male (58%) and Caucasian (92%) with clinical stage III disease (68%). Seventy-three patients (81%) underwent low anterior resection (LAR), 17 (19%) underwent abdominoperineal resection (APR). The median interval from completion of nCRT to surgery was 62 days (IQR: 56-70 days). The 4-year OS, DFS, and LC was 92.4%, 74.4%, and 90.2%, respectively. In the multivariate analysis, ypTN downstaging was not prognostically significant; however, AJCC TRG score 3 (minimal tumor response to treatment) was strongly predictive for inferior DFS (3-year DFS 79% vs. 25%, P<0.001). Patients with TRG 3 had a significantly higher risk of both local (75% vs. 5%) and distant failure (75% vs. 19%).
Conclusions: Minimal tumor response to neoadjuvant therapy, AJCC TRG 3, irrespective of ypTN downstaging, is a pattern of residual disease that is at highest risk for recurrence. Response categorization discrepancies may be partly explained by alternative patterns of residual disease, including tumor fragmentation, and may be best reflected by TRG. The optimal tumor response categorization method requires further study to best stratify patient risk and management.
Keywords: Rectal cancer; downstaging; neoadjuvant chemoradiation (nCRT); tumor regression grading (TRG).
2022 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-22-477/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- NCCN Clinical Practice Guidelines in Oncology: Rectal Cancer. In: Version 2.2021. 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf
LinkOut - more resources
Full Text Sources
Miscellaneous