

Predictive performance of interferon-gamma release assays and the tuberculin skin test for incident tuberculosis: an individual participant data meta-analysis
- PMID: 36636295
- PMCID: PMC9829704
- DOI: 10.1016/j.eclinm.2022.101815
Predictive performance of interferon-gamma release assays and the tuberculin skin test for incident tuberculosis: an individual participant data meta-analysis
Abstract
Background: Evidence on the comparative performance of purified protein derivative tuberculin skin tests (TST) and interferon-gamma release assays (IGRA) for predicting incident active tuberculosis (TB) remains conflicting. We conducted an individual participant data meta-analysis to directly compare the predictive performance for incident TB disease between TST and IGRA to inform policy.
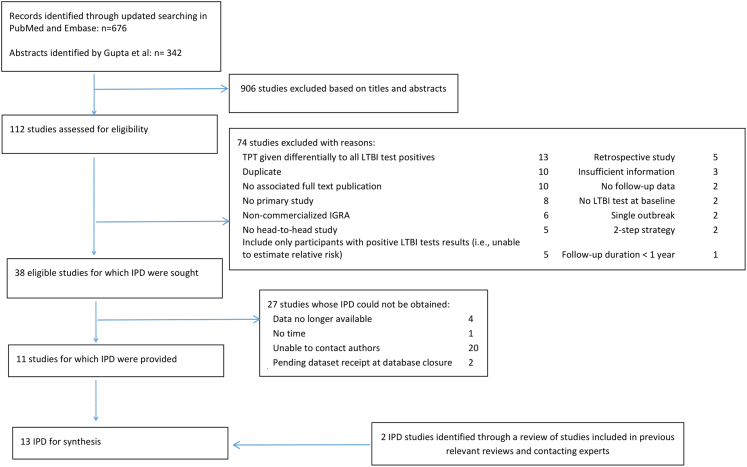
Methods: We searched Medline and Embase from 1 January 2002 to 4 September 2020, and studies that were included in previous systematic reviews. We included prospective longitudinal studies in which participants received both TST and IGRA and estimated performance as hazard ratios (HR) for the development of all diagnoses of TB in participants with dichotomised positive test results compared to negative results, using different thresholds of positivity for TST. Secondary analyses included an evaluation of the impact of background TB incidence. We also estimated the sensitivity and specificity for predicting TB. We explored heterogeneity through pre-defined sub-group analyses (e.g. country-level TB incidence). Publication bias was assessed using funnel plots and Egger's test. This review is registered with PROSPERO, CRD42020205667.
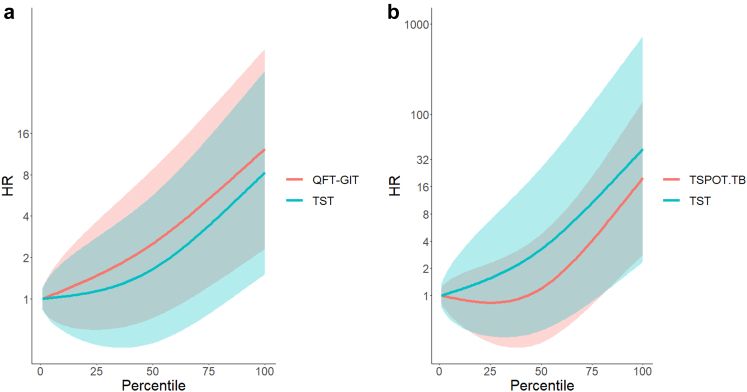
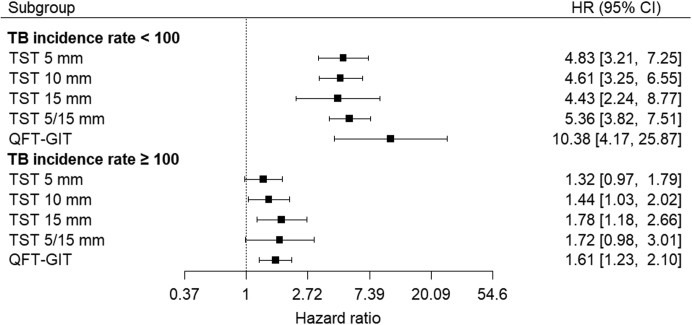
Findings: We obtained data from 13 studies out of 40 that were considered eligible (N = 32,034 participants: 36% from countries with TB incidence rate ≥100 per 100,000 population). All reported data on TST and QuantiFERON Gold in-Tube (QFT-GIT). The point estimate for the TST was highest with higher cut-offs for positivity and particularly when stratified by bacillus Calmette-Guérin vaccine (BCG) status (15 mm if BCG vaccinated and 5 mm if not [TST5/15 mm]) at 2.88 (95% CI 1.69-4.90). The pooled HR for QFT-GIT was higher than for TST at 4.15 (95% CI 1.97-8.75). The difference was large in countries with TB incidence rate <100 per 100,000 population (HR 10.38, 95% CI 4.17-25.87 for QFT-GIT VS. HR 5.36, 95% CI 3.82-7.51 for TST5/15 mm) but much of this difference was driven by a single study (HR 5.13, 95% CI 3.58-7.35 for TST5/15 mm VS. 7.18, 95% CI 4.48-11.51 for QFT-GIT, when excluding the study, in which all 19 TB cases had positive QFT-GIT results). The comparative performance was similar in the higher burden countries (HR 1.61, 95% CI 1.23-2.10 for QFT-GIT VS. HR 1.72, 95% CI 0.98-3.01 for TST5/15 mm). The predictive performance of both tests was higher in countries with TB incidence rate <100 per 100,000 population. In the lower TB incidence countries, the specificity of TST (76% for TST5/15 mm) and QFT-GIT (74%) for predicting active TB approached the minimum World Health Organization target (≥75%), but the sensitivity was below the target of ≥75% (63% for TST5/15 mm and 65% for QFT-GIT). The absolute differences in positive and negative predictive values between TST15 mm and QFT-GIT were small (positive predictive values 2.74% VS. 2.46%; negative predictive values 99.42% VS. 99.52% in low-incidence countries). Egger's test did not show evidence of publication bias (0.74 for TST15 mm and p = 0.68 for QFT-GIT).
Interpretation: IGRA appears to have higher predictive performance than the TST in low TB incidence countries, but the difference was driven by a single study. Any advantage in clinical performance may be small, given the numerically similar positive and negative predictive values. Both IGRA and TST had lower performance in countries with high TB incidence. Test choice should be contextual and made considering operational and likely clinical impact of test results.
Funding: YH, IA, and MXR were supported by the National Institute for Health and Care Research (NIHR), United Kingdom (RP-PG-0217-20009). MQ was supported by the Medical Research Council [MC_UU_00004/07].
Keywords: IGRA; LTBI; Prevention; Prophylaxis; Tuberculin skin test.
© 2022 The Author(s).
Conflict of interest statement
YH and MXR report donation of QIAreach, an IGRA, by QIAGEN for a LTBI infection survey. YH, MXR, and IA report donations of Cy-TB, a TB-specific skin test for detection of LTBI, by the Serum Institute of India for a study on the feasibility and patient-important outcomes. They had no role in the submitted work. RD declared the receipt of payment for lectures from Qiagen and Oxford Immunotec. JD declared honoraria for lectures from Oxford Immunotec. AG declared receipt of research grants from the US National Institute of Health (NIH) and membership in NIH Council and IndoUS Science Technology Forum. CL provided consultation service to INSMED and received speakers honoraria from INSMED, GILEAD, JANSSEN and is a member of the Data Safety Board of trials from Medicines sans Frontiers, all outside of the submitted work. ILR has a patent (PCT/EP2019/064885), in vitro method for the diagnosis or detection of non-tuberculous mycobacteria. MS reports receipt of test kits free of charge from Qiagen and Oxford Immunotec. MS also reports receipt of research grants from Biotest and Astellas, consulting fees and honoraria from Biotest, Moderna, Qiagen, and Takeda, support for travel from Biotest, and participation on advisory board for Biotest and Moderna, all outside of this work. GS reports receipt of consulting fees from Pfizer, Diasorin, and INSMED. All other authors declare no competing interests.
Figures
References
-
- World Health Organization . WHO; Geneva, Switzerland: 2020. WHO consolidated guidelines on tuberculosis: module 1: prevention: tuberculosis preventive treatment. - PubMed
-
- Mack U., Migliori G.B., Sester M., et al. LTBI: latent tuberculosis infection or lasting immune responses to M. tuberculosis? A TBNET consensus statement. Eur Respir J. 2009;33(5):956–973. - PubMed
-
- Latent tuberculosis infection: updated and consolidated guidelines for programmatic management. WHO; Geneva, Switzerland: 2018. - PubMed
-
- Zhou G., Luo Q., Luo S., et al. Interferon-gamma release assays or tuberculin skin test for detection and management of latent tuberculosis infection: a systematic review and meta-analysis. Lancet Infect Dis. 2020;20:1457. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
