

Biomarker Trends, Incidence, and Outcomes of Immune Checkpoint Inhibitor-Induced Myocarditis
- PMID: 36636441
- PMCID: PMC9830199
- DOI: 10.1016/j.jaccao.2022.11.004
Biomarker Trends, Incidence, and Outcomes of Immune Checkpoint Inhibitor-Induced Myocarditis
Abstract
Background: Myocarditis is a dreaded and unpredictable complication of immune checkpoint inhibitors (ICI). We sought to determine whether routinely measured biomarkers could be helpful in monitoring for ICI myocarditis.
Objectives: The authors examined biomarker trends of patients on ICI and their association with the incidence of ICI myocarditis and outcomes.
Methods: We conducted an observational cohort study of adults who received at least one dose of ICI at Michigan Medicine between June 2014 and December 2021 and underwent systematic serial testing for aspartate aminotransferase (AST) and alanine aminotransferase (ALT), creatine phosphokinase (CPK), and lactate dehydrogenase during ICI therapy.
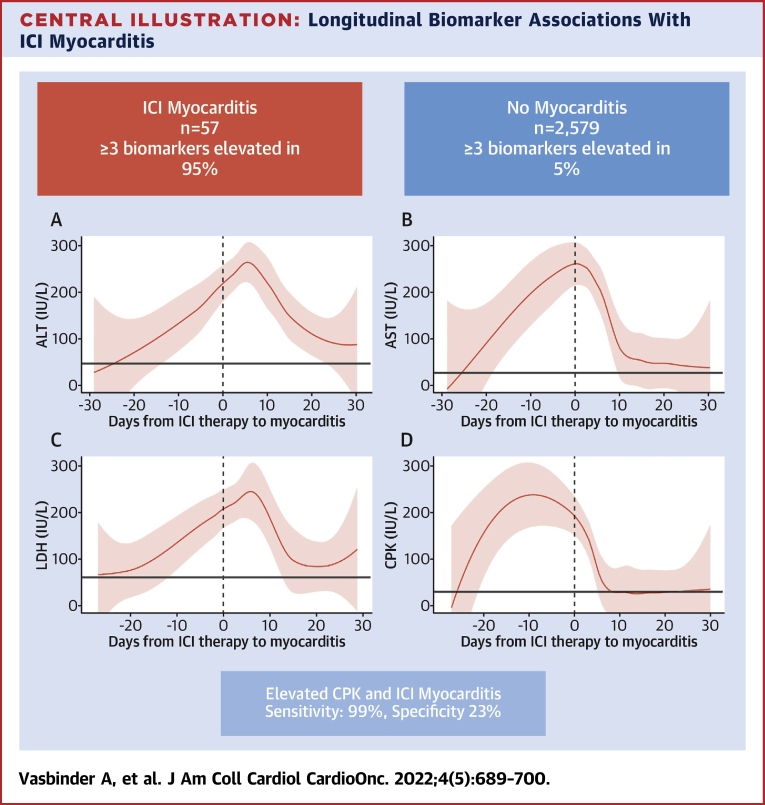
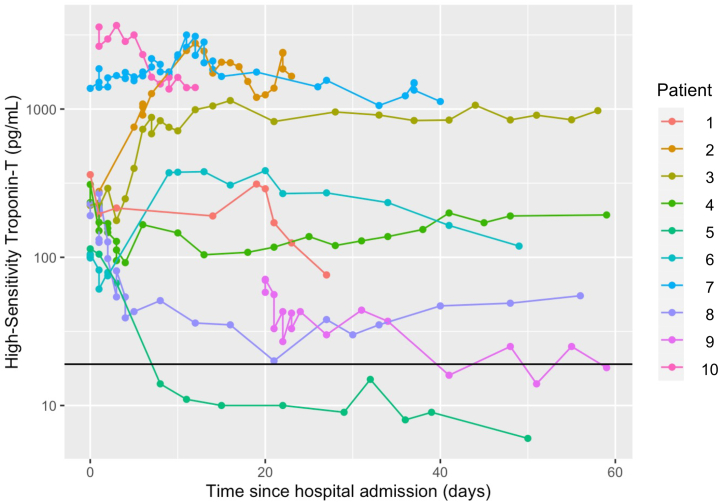
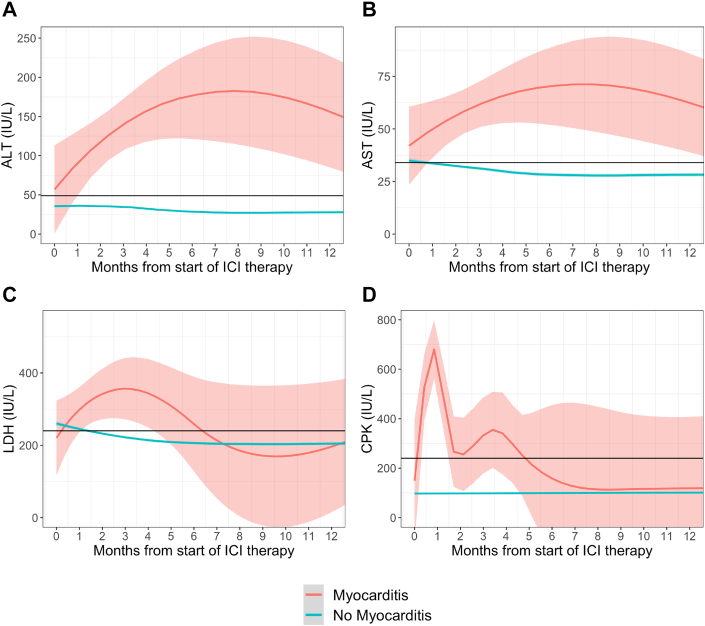
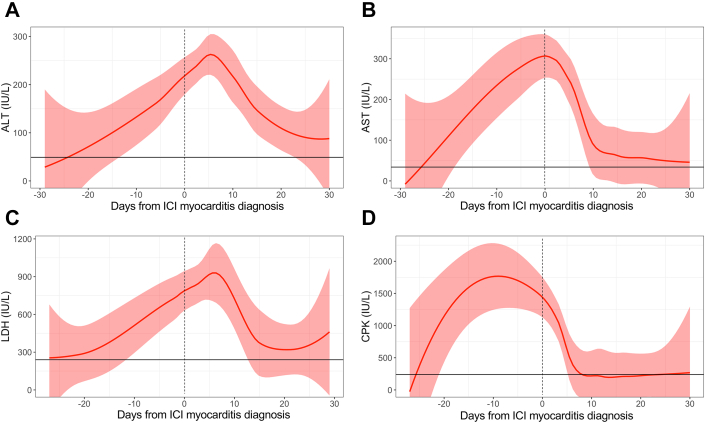
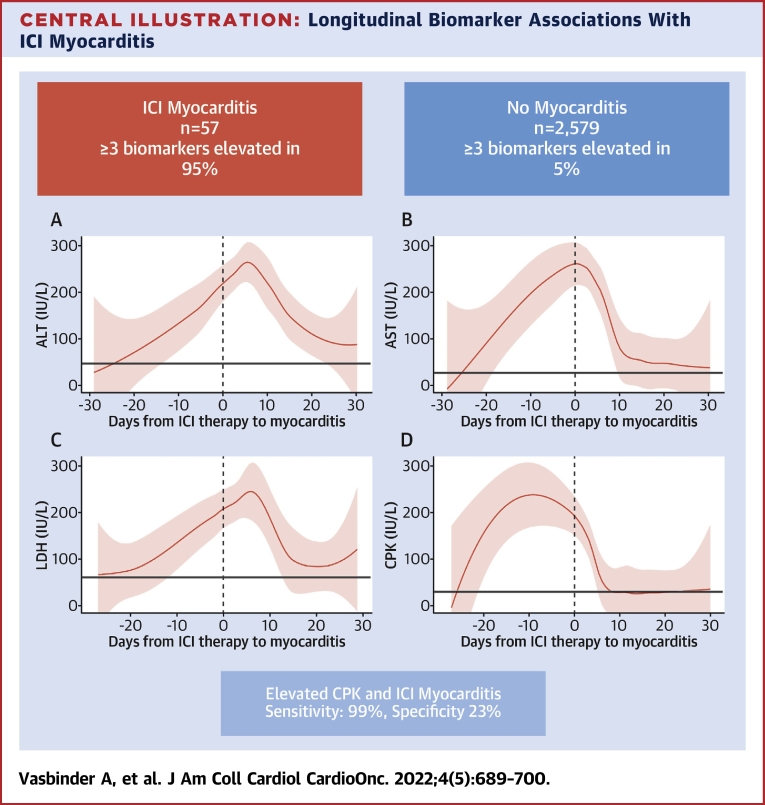
Results: Among 2,606 patients (mean age 64 ± 13 years; 60.7% men), 27 (1.0%) were diagnosed with ICI myocarditis. At diagnosis, patients with myocarditis had an elevated high-sensitivity troponin T (100%), ALT (88.9%), AST (85.2%), CPK (88.9%), and lactate dehydrogenase (92.6%). Findings were confirmed in an independent cohort of 30 patients with biopsy-confirmed ICI myocarditis. A total of 95% of patients with ICI myocarditis had elevations in at least 3 biomarkers compared with 5% of patients without myocarditis. Among the noncardiac biomarkers, only CPK was associated (per 100% increase) with the development of myocarditis (HR: 1.83; 95% CI: 1.59-2.10) and all-cause mortality (HR: 1.10; 95% CI: 1.01-1.20) in multivariable analysis. Elevations in CPK had a sensitivity of 99% and specificity of 23% for identifying myocarditis.
Conclusions: ICI myocarditis is associated with changes in AST, ALT, and CPK. An increase in noncardiac biomarkers during ICI treatment, notably CPK, should prompt further evaluation for ICI myocarditis.
Keywords: ALT; ALT, alanine aminotransferase; AST; AST, aspartate aminotransferase; CPK; CPK, creatine phosphokinase; ICI, immune checkpoint inhibitor; LDH, lactate dehydrogenase; ULN, upper limit of normal; biomarkers; hsTnT, high-sensitivity troponin T; immune checkpoint inhibitor; immunotherapy; irAE, immune-related adverse event; myocarditis; troponin.
© 2022 The Authors.
Conflict of interest statement
Dr Vasbinder is supported by a National Heart, Lung, and Blood Institute funded postdoctoral fellowship (T32HL007853). Dr Hayek is supported by National Heart, Lung, and Blood Institute (R01HL153384) and the National Institute on Diabetes and Digestive and Kidney Diseases (R01-DK128012). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Wolchok J. Putting the immunologic brakes on cancer. Cell. 2018;175:1452–1454. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
