

Immune Checkpoint Inhibitor Therapy in Oncology: Current Uses and Future Directions: JACC: CardioOncology State-of-the-Art Review
- PMID: 36636451
- PMCID: PMC9830229
- DOI: 10.1016/j.jaccao.2022.09.004
Immune Checkpoint Inhibitor Therapy in Oncology: Current Uses and Future Directions: JACC: CardioOncology State-of-the-Art Review
Abstract
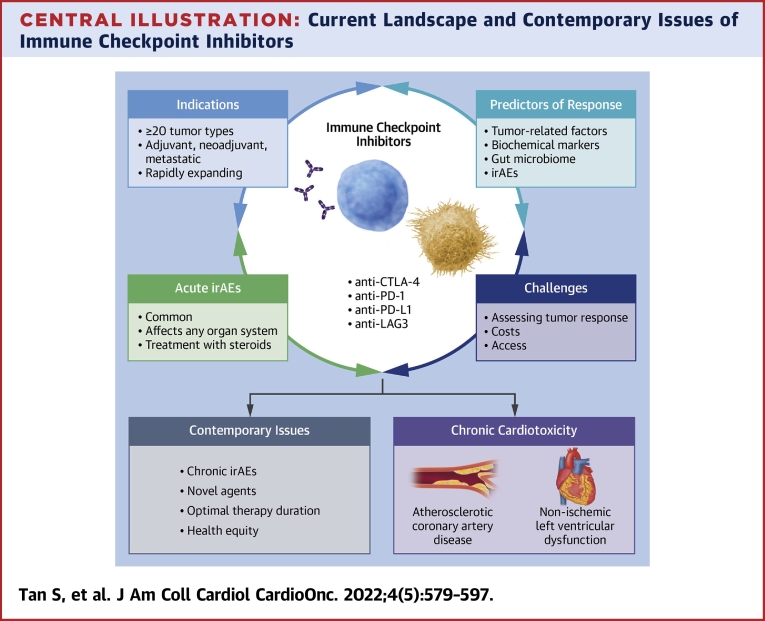
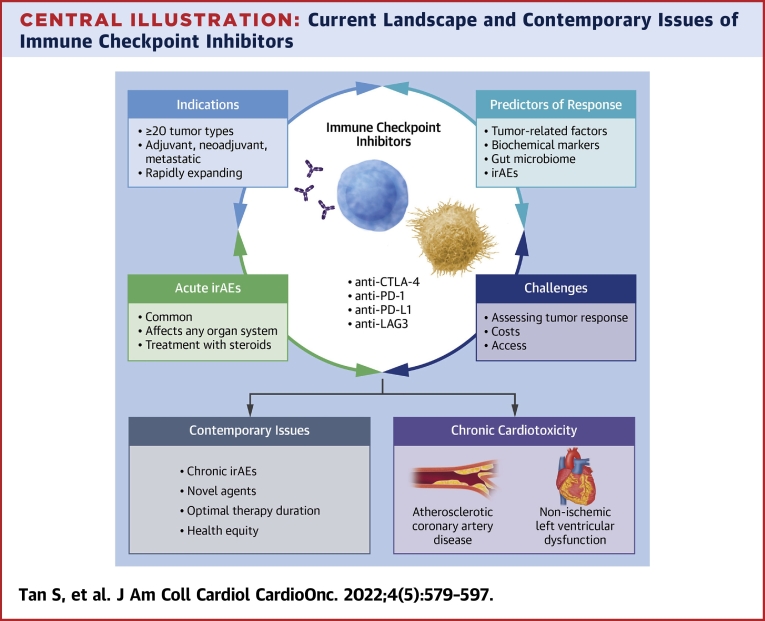
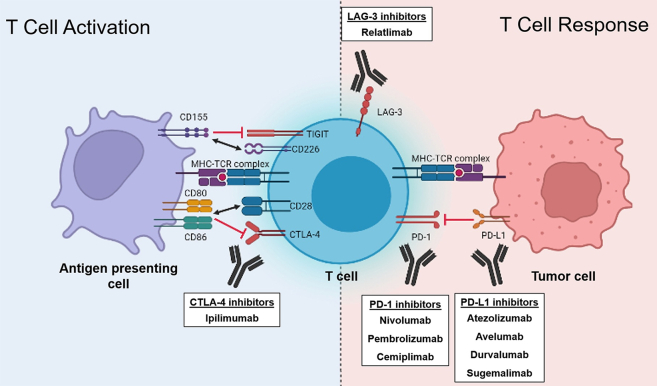
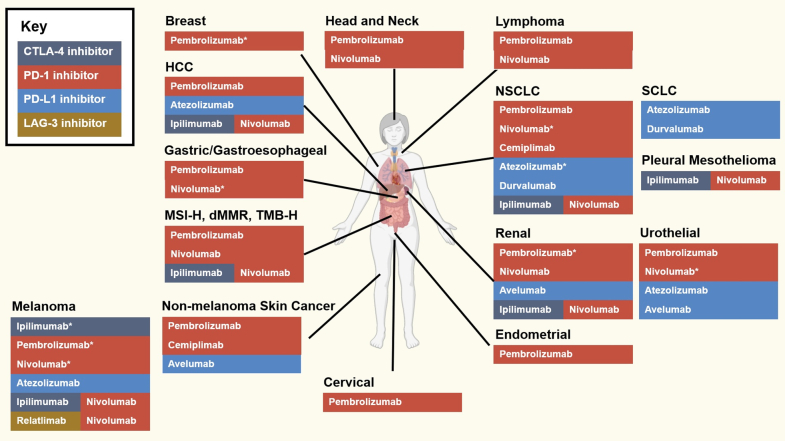
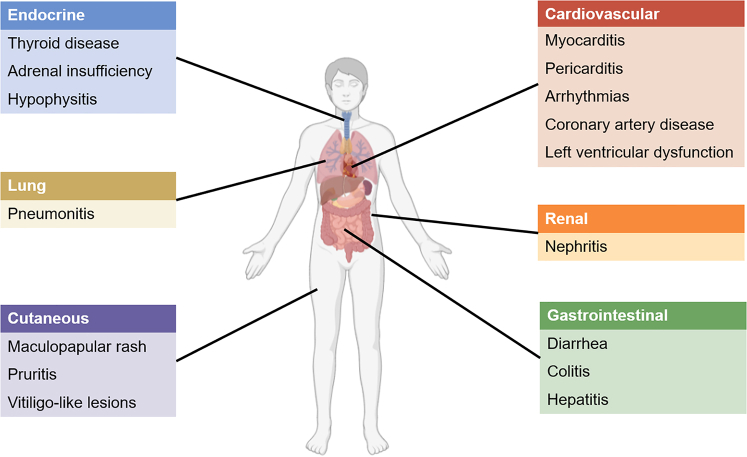
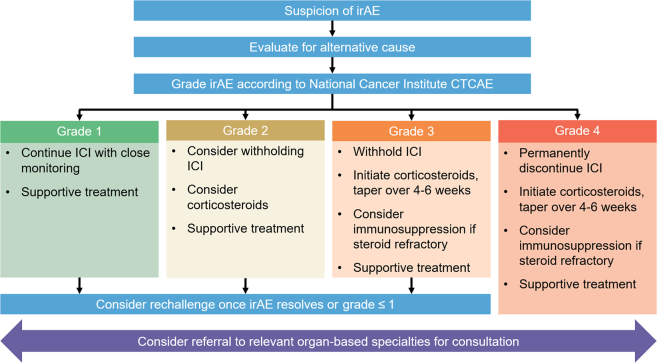
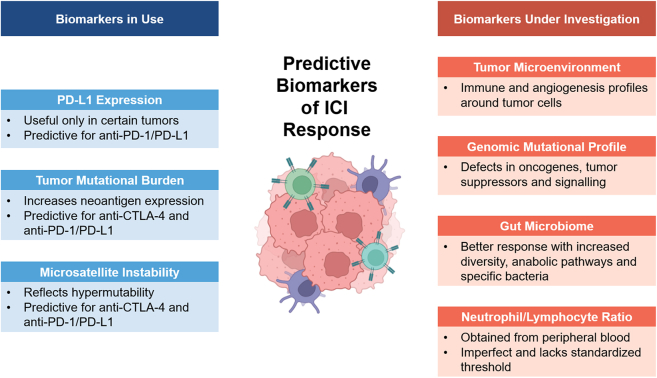
Immune checkpoint inhibitors (ICIs) are a major class of immuno-oncology therapeutics that have significantly improved the prognosis of various cancers, both in (neo)adjuvant and metastatic settings. Unlike other conventional therapies, ICIs elicit antitumor effects by enhancing host immune systems to eliminate cancer cells. There are 3 approved ICI classes by the U.S. Food and Drug Administration: inhibitors targeting cytotoxic T lymphocyte associated antigen 4, programmed death 1/programmed death-ligand 1, and lymphocyte-activation gene 3, with many more in development. ICIs are commonly associated with distinct toxicities, known as immune-related adverse events, which can arise during treatment or less frequently be of late onset, usually relating to excessive activation of the immune system. Acute cardiovascular immune-related adverse events such as myocarditis are rare; however, data suggesting chronic cardiovascular sequelae are emerging. This review presents the current landscape of ICIs in oncology, with a focus on important aspects relevant to cardiology.
Keywords: CTLA-4, cytotoxic T lymphocyte associated antigen 4; ICI, immune checkpoint inhibitors; LAG-3, lymphocyte-activation gene 3; MSI, microsatellite instability; PD-L1, programmed death-ligand 1; TMB, tumor mutational burden; TME, tumor microenvironment; biomarkers; cardio-oncology; cardiotoxicity; immune checkpoint inhibitors; immune related adverse events; immunotherapy; irAE, immune-related adverse event; medical oncology.
© 2022 The Authors.
Conflict of interest statement
Dr Tan is supported by a postgraduate scholarship from the National Health and Medical Research Council of Australia, a PhD scholarship from the National Heart Foundation of Australia, and an Australian Government Research Training Program Scholarship. Dr Day is a recipient of the Royal Australasian College of Physicians Foundation 2022 Basser Research Entry Scholarship; and has received research support (clinical trials for the institution) from Beigene, Bristol-Myers Squibb, EpimAb, Harbour BioMed, Maxinovel, MSD, Olema Pharmaceuticals, Pfizer, PhamAbcine, and Roche. Dr Nicholls has received research support from AstraZeneca, Amgen, Anthera, CSL Behring, Cerenis, Eli Lilly, Esperion, Resverlogix, Novartis, InfraReDx, and Sanofi-Regeneron; and served as a consultant for Amgen, Akcea, AstraZeneca, Boehringer Ingelheim, CSL Behring, Eli Lilly, Esperion, Kowa, Merck, Takeda, Pfizer, Sanofi-Regeneron, and Novo Nordisk. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Ledford H., Else H., Warren M. Cancer immunologists scoop medicine Nobel prize. Nature. 2018;562:20–21. - PubMed
-
- Negrier S., Escudier B., Lasset C., et al. Recombinant human interleukin-2, recombinant human interferon alfa-2a, or both in metastatic renal-cell carcinoma. Groupe Francais d'Immunotherapie. N Engl J Med. 1998;338:1272–1278. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
