

Management of anastomotic leakage after robot-assisted minimally invasive esophagectomy with an intrathoracic anastomosis
- PMID: 36636758
- PMCID: PMC10226267
- DOI: 10.1093/dote/doac094
Management of anastomotic leakage after robot-assisted minimally invasive esophagectomy with an intrathoracic anastomosis
Abstract
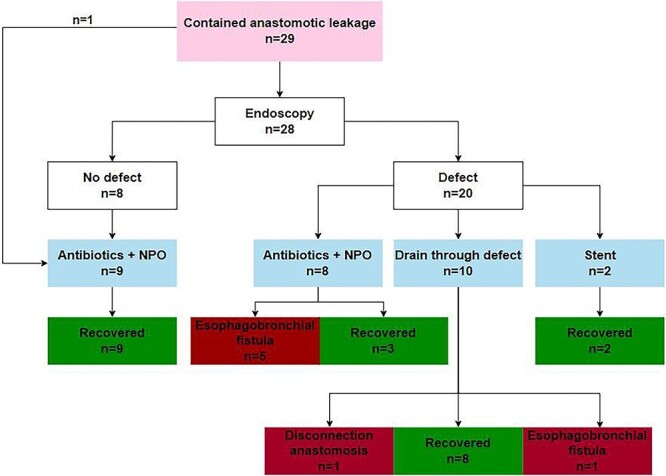
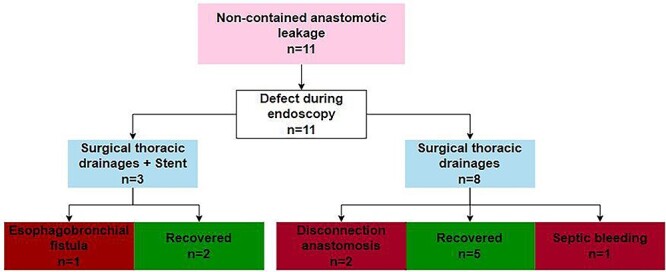
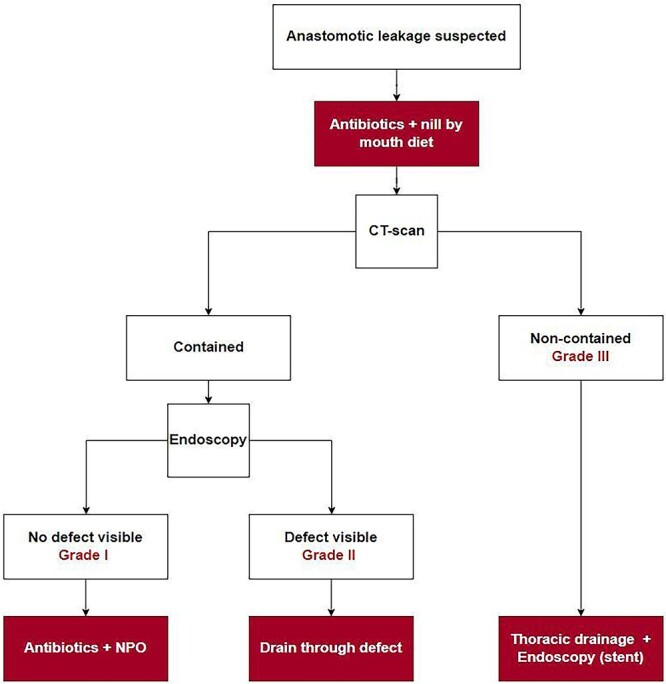
Anastomotic leakage is a feared complication after esophagectomy and associated with increased post-operative morbidity and mrotality. The aim of this study was to evaluate the management of leakage after robot-assisted minimally invasive esophagectomy (RAMIE) with intrathoracic anastomosis. From a single center prospectively maintained database, all patients with anastomotic leakages defined by the Esophageal Complications Consensus Group between 2016 and 2021 were included. Contained leakage was defined as presence of air or fluid at level of the anastomosis without the involvement of the mediastinum or thorax. Non-contained leakage was defined as mediastinitis and/or mediastinal/pleural fluid collections. The primary outcome was 90-day mortality and the secondary outcome was successful recovery. In this study, 40 patients with anastomotic leakage were included. The 90-day mortality rate was 3% (n = 1). Leakage was considered contained in 29 patients (73%) and non-contained in 11 patients (27%). In the contained group, the majority of the patients were treated non-surgically (n = 27, 93%) and management was successful in 22 patients (76%). In the non-contained group, all patients required a reoperation with thoracic drainage and management was successful in seven patients (64%). Management failed in 11 patients (28%) of whom 7 developed an esophagobronchial fistula, 3 had a disconnection of the anastomosis and 1 died of a septic bleeding. In conclusion, this study demonstrates that the management anastomotic leakage in patients who underwent RAMIE with an intrathoracic anastomosis was successful in 73% of the patients with a 90-day mortality rate of 3%. A differentiated approach for the management of intrathoracic anastomotic leakage is proposed.
Keywords: Robotic surgery; anastomotic leakage; esophagectomy; treatment.
© The Author(s) 2023. Published by Oxford University Press on behalf of International Society for Diseases of the Esophagus.
Conflict of interest statement
Richard van Hillegersberg and Jelle Ruurda are proctors for Intuitive Surgical Inc and consultants for Medtronic. Eline de Groot, Sebastiaan Bronzwaer, Lucas Goense, Feike Kingma, Sylvia van der Horst and Jan Willem van den Berg have no conflicts of interest to declare.
Figures
References
-
- Haverkamp L, Seesing M F J, Ruurda J P, Boone J, van Hillegersberg R. Worldwide trends in surgical techniques in the treatment of esophageal and gastroesophageal junction cancer. Dis Esophagus 2017; 30(1): 1–7. - PubMed
-
- van der Sluis P C, van der Horst S, May A M, Schippers C, Brosens L A A, Joore H C A et al. Robot-assisted minimally invasive thoracolaparoscopic esophagectomy versus open transthoracic esophagectomy for resectable esophageal cancer: a randomized controlled trial. Ann Surg 2019; 269(4): 621–30. - PubMed
-
- Straatman J, Van Der Wielen N, Cuesta M A, Daams F, Roig Garcia J, Bonavina L et al. Minimally invasive versus open esophageal resection. Ann Surg 2017. - PubMed
-
- Low D E, Kuppusamy M K, Alderson D, Cecconello I, Chang A C, Darling G et al. Benchmarking complications associated with esophagectomy. Ann Surg 2019; 269(2): 291–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
