

Analysis of Psychological Symptoms Following Disclosure of Amyloid-Positron Emission Tomography Imaging Results to Adults With Subjective Cognitive Decline
- PMID: 36637820
- PMCID: PMC9857261
- DOI: 10.1001/jamanetworkopen.2022.50921
Analysis of Psychological Symptoms Following Disclosure of Amyloid-Positron Emission Tomography Imaging Results to Adults With Subjective Cognitive Decline
Erratum in
-
Error in Supplement 2.JAMA Netw Open. 2023 Mar 1;6(3):e235066. doi: 10.1001/jamanetworkopen.2023.5066. JAMA Netw Open. 2023. PMID: 36884255 Free PMC article. No abstract available.
Abstract
Importance: Individuals who are amyloid-positive with subjective cognitive decline and clinical features increasing the likelihood of preclinical Alzheimer disease (SCD+) are at higher risk of developing dementia. Some individuals with SCD+ undergo amyloid-positron emission tomography (PET) as part of research studies and frequently wish to know their amyloid status; however, the disclosure of a positive amyloid-PET result might have psychological risks.
Objective: To assess the psychological outcomes of the amyloid-PET result disclosure in individuals with SCD+ and explore which variables are associated with a safer disclosure in individuals who are amyloid positive.
Design, setting, and participants: This prospective, multicenter study was conducted as part of The Amyloid Imaging to Prevent Alzheimer Disease Diagnostic and Patient Management Study (AMYPAD-DPMS) (recruitment period: from April 2018 to October 2020). The setting was 5 European memory clinics, and participants included patients with SCD+ who underwent amyloid-PET. Statistical analysis was performed from July to October 2022.
Exposures: Disclosure of amyloid-PET result.
Main outcomes and measures: Psychological outcomes were defined as (1) disclosure related distress, assessed using the Impact of Event Scale-Revised (IES-R; scores of at least 33 indicate probable presence of posttraumatic stress disorder [PTSD]); and (2) anxiety and depression, assessed using the Hospital Anxiety and Depression scale (HADS; scores of at least 15 indicate probable presence of severe mood disorder symptoms).
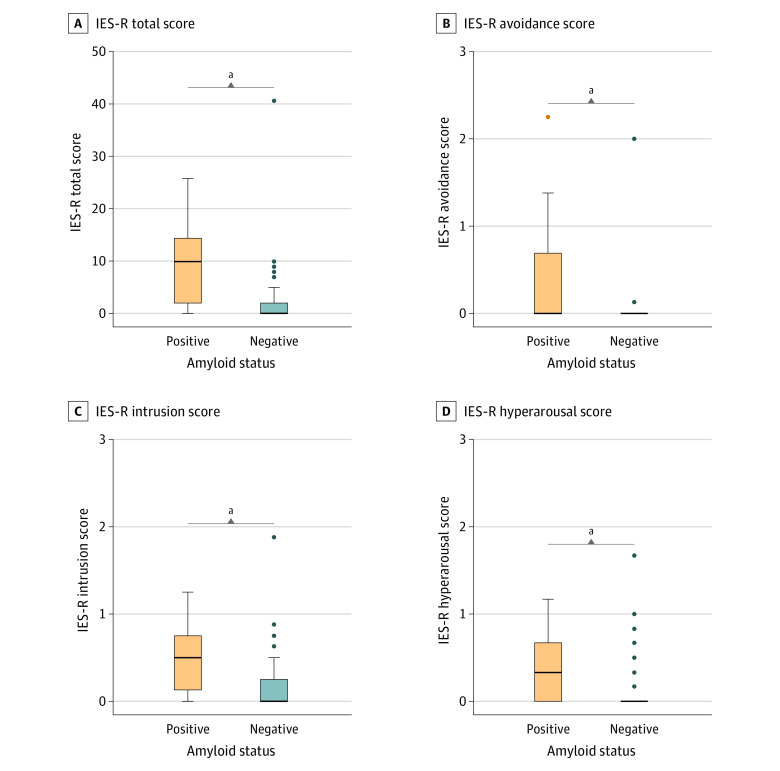
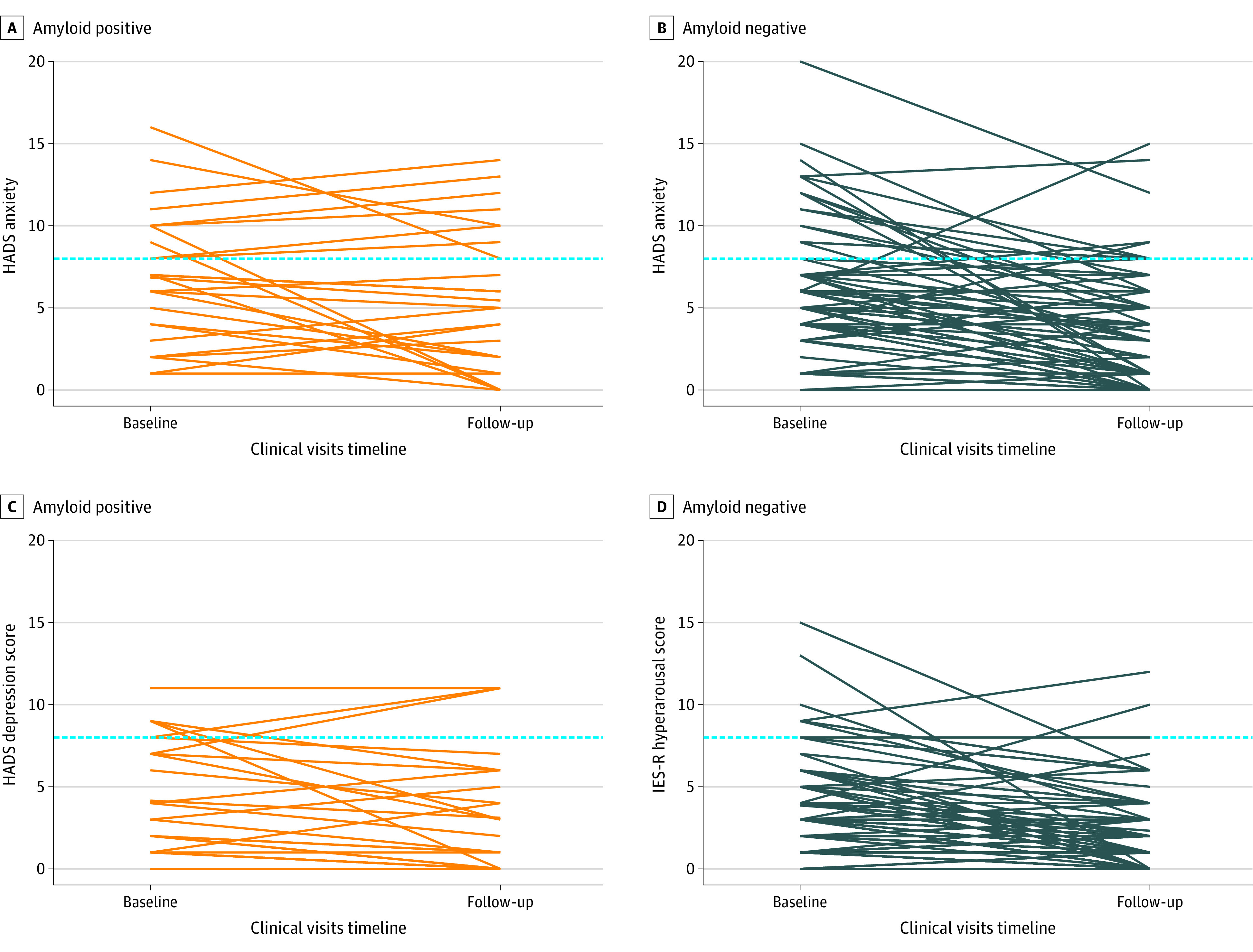
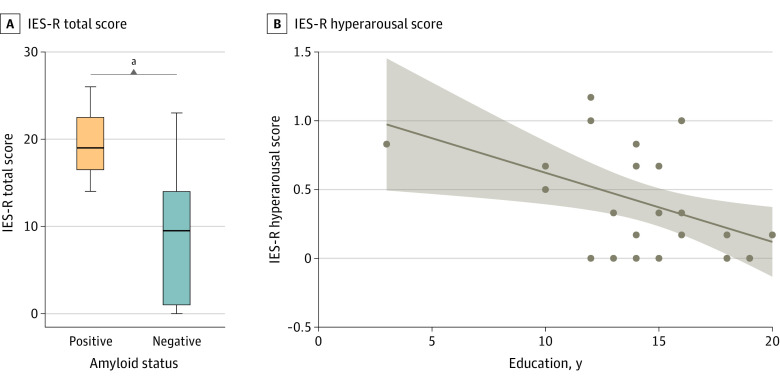
Results: After disclosure, 27 patients with amyloid-positive SCD+ (median [IQR] age, 70 [66-74] years; gender: 14 men [52%]; median [IQR] education: 15 [13 to 17] years, median [IQR] Mini-Mental State Examination [MMSE] score, 29 [28 to 30]) had higher median (IQR) IES-R total score (10 [2 to 14] vs 0 [0 to 2]; P < .001), IES-R avoidance (0.00 [0.00 to 0.69] vs 0.00 [0.00 to 0.00]; P < .001), IES-R intrusions (0.50 [0.13 to 0.75] vs 0.00 [0.00 to 0.25]; P < .001), and IES-R hyperarousal (0.33 [0.00 to 0.67] vs 0.00 [0.00 to 0.00]; P < .001) scores than the 78 patients who were amyloid-negative (median [IQR], age, 67 [64 to 74] years, 45 men [58%], median [IQR] education: 15 [12 to 17] years, median [IQR] MMSE score: 29 [28 to 30]). There were no observed differences between amyloid-positive and amyloid-negative patients in the median (IQR) HADS Anxiety (-1.0 [-3.0 to 1.8] vs -2.0 [-4.8 to 1.0]; P = .06) and Depression (-1.0 [-2.0 to 0.0] vs -1.0 [-3.0 to 0.0]; P = .46) deltas (score after disclosure - scores at baseline). In patients with amyloid-positive SCD+, despite the small sample size, higher education was associated with lower disclosure-related distress (ρ = -0.43; P = .02) whereas the presence of study partner was associated with higher disclosure-related distress (W = 7.5; P = .03). No participants with amyloid-positive SCD+ showed probable presence of PTSD or severe anxiety or depression symptoms at follow-up.
Conclusions and relevance: The disclosure of a positive amyloid-PET result to patients with SCD+ was associated with a bigger psychological change, yet such change did not reach the threshold for clinical concern.
Conflict of interest statement
Figures
Comment in
-
Clinical Practice in the Alzheimer Biomarker Era-Drugs for the Brain and Care for the Mind.JAMA Netw Open. 2023 Jan 3;6(1):e2250938. doi: 10.1001/jamanetworkopen.2022.50938. JAMA Netw Open. 2023. PMID: 36637828 Free PMC article. No abstract available.
References
-
- Johnson KA, Minoshima S, Bohnen NI, et al. ; Alzheimer’s Association; Society of Nuclear Medicine and Molecular Imaging; Amyloid Imaging Taskforce . Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimers Dement. 2013;9(1):e-1-e-16. doi:10.1016/j.jalz.2013.01.002 - DOI - PMC - PubMed
-
- Johnson KA, Minoshima S, Bohnen NI, et al. ; Amyloid Imaging Task Force of the Alzheimer’s Association and Society for Nuclear Medicine and Molecular Imaging . Update on appropriate use criteria for amyloid PET imaging: dementia experts, mild cognitive impairment, and education. Alzheimers Dement. 2013;9(4):e106-e109. doi:10.1016/j.jalz.2013.06.001 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
