

Geriatric assessment and the variance of treatment recommendations in geriatric patients with gastrointestinal cancer-a study in AIO oncologists
- PMID: 36638708
- PMCID: PMC10024156
- DOI: 10.1016/j.esmoop.2022.100761
Geriatric assessment and the variance of treatment recommendations in geriatric patients with gastrointestinal cancer-a study in AIO oncologists
Abstract
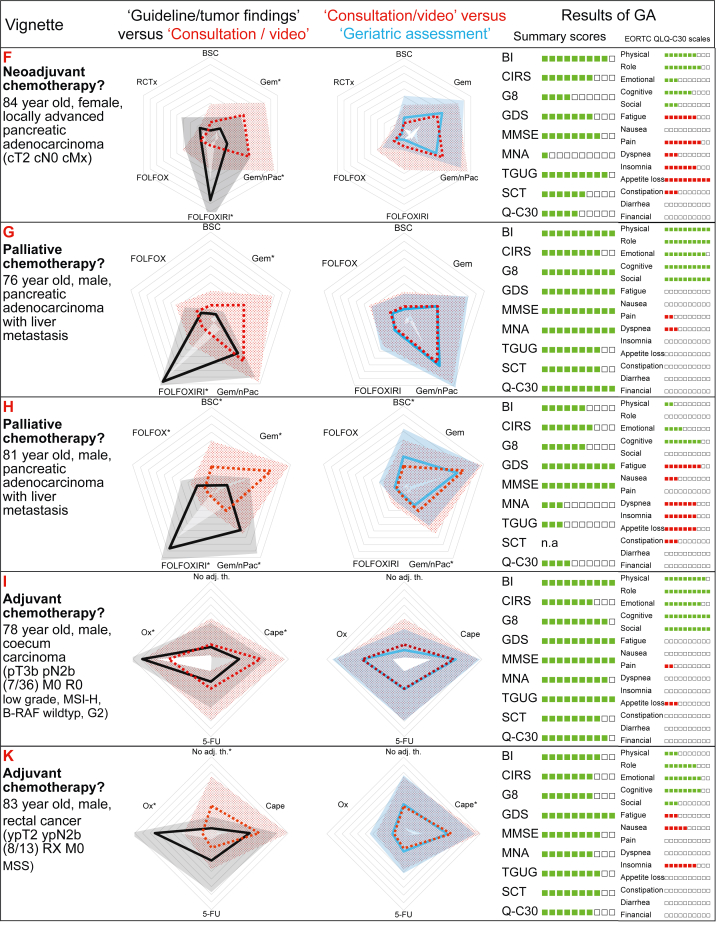
Background: Geriatric assessment (GA) is recommended to detect vulnerabilities for elderly cancer patients. To assess whether results of GA actually influence the treatment recommendations, we conducted a case vignette-based study in medical oncologists.
Materials and methods: Seventy oncologists gave their medical treatment recommendations for a maximum of 4 out of 10 gastrointestinal cancer patients in three steps: (i) based on tumor findings alone to simulate the guideline recommendation for a '50-year-old standard patient without comorbidities'; (ii) for the same situation in elderly patients (median age 77.5 years) according to the comorbidities, laboratory values and a short video simulating the clinical consultation; and (iii) after the results of a full GA including interpretation aid [Barthel Index, Cumulative Illness Rating Scale (CIRS), Geriatric 8 (G8), Geriatric Depression Scale (GDS), Mini Mental Status Examination (MMSE), Mini-Nutritional Assessment (MNA), Timed Get Up and Go (TGUG), European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-30 (EORTC QLQ-C30), stair climb test].
Results: Data on 164 treatment recommendations were analyzed. The recommendations had a significantly higher variance for elderly patients than for 'standard' patients (944 versus 602, P < 0.0001) indicating a lower agreement between oncologists. Knowledge on GA had marginal influence on the treatment recommendation or its variance (944 versus 940, P = 0.92). There was no statistically significant influence of the working place or the years of experience in oncology on the variance of recommendations. The geriatric tools were rated approximately two times higher as being 'meaningful' (53%) and 'useful for the presented cases' (49%) than they were 'used in clinical practice' (19%). The most commonly used geriatric tool in patient care was the MNA (30%).
Conclusions: The higher variance of treatment recommendations indicates that it is less likely for elderly patients to get the optimal recommendation. Although the proposed therapeutic regimen varied higher in elderly patients and the oncologists rated the GA results as 'useful', the GA results did not influence the individual recommendations or its variance. Continuing education on GA and research on implementation into clinical practice are needed.
Keywords: chemotherapy; geriatric assessment; geriatric oncology; survey.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Funding This work was supported by the institution (Technical University Dresden/University Hospital Carl Gustav Carus). There was no additional funding.
Figures




References
-
- Robert Koch-Institut Krebs in Deutschland für 2017/2018 [Cancer in Germany 2017/2018] Robert Koch-Institut und Gesellschaft der epidemiologischen Krebsregister in Deutschland e.V; Berlin: 2021.
-
- Smith B.D., Smith G.L., Hurria A., Hortobagyi G.N., Buchholz T.A. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol. 2009;27(17):2758–2765. - PubMed
-
- Trimble E.L., Carter C.L., Cain D., Freidlin B., Ungerleider R.S., Friedman M.A. Representation of older patients in cancer treatment trials. Cancer. 1994;74(7):2208–2214. - PubMed
-
- Hutchins L.F., Unger J.M., Crowley J.J., Coltman C.A., Jr., Albain K.S. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N Engl J Med. 1999;341(27):2061–2067. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
